Integrated Abutment Crown™ (IAC): Seating Techniques
Page 1 | Page 2 | Page 3 | Page 4 | Page 5 | Page 6 | Page 7 | Page 8 | Page 9 | Page 10 | Page 11 | Page 12
Seating of an Integrated Abutment Crown (IAC)
 |
 |
 |
 |
 |
 |
 |
 |
1. Remove the transitional crown or temporary abutment, wipe the post of the IAC clean with alcohol and place the IAC into the well of the implant.
2. Use an incisal orientation jig or vacuum formed template to assure proper anatomical alignment. Initially, confirm occlusal and passive interproximal contacts. Often a slight rotation of an IAC will close or open an interproximal contact.
3.Since IACs should be fabricated with ideal emergence contours without the use of ridge laps, tissue contours may inhibit their proper seating. Often it is necessary to make two oblique crestal relieving incisions that will allow the IAC to displace the soft tissue while it is being seated.
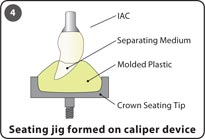
4.It is essential to tap the IAC in the long axis of the abutment post and implant well in order to engage the frictional locking taper connection without distorting the roundness of the abutment post and implant well. If the angle of the crown is such that while tapping on the incisal edge you are not applying force in the long axis of the post, fabricate a seating jig by using a caliper alignment device and a crown seating tip.
5. Using a 250g mallet, tap the crown into place with a few taps. Use a plastic healing abutment, or more ideally a seating jig to facilitate the seating of an IAC. Refrain from tapping directly on the incisal edge of the crown with a sharp object. A posterior IAC may be seated by simply having the patient close onto the restoration.
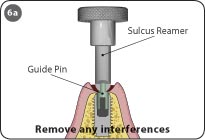
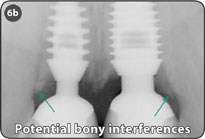
6. Prior to seating some IACs, it may be necessary to use a guide pin and a sulcus reamer to remove any bony interferences. Potential bony interferences may be seen on a radiograph.
Note: The use of a seating jig which was fabricated with a caliper alignment device is recommended for maxillary anterior IACs.
Keys to Success
- Extreme care must be given to the evaluation and adjustments of the interproximal contacts for maxillary anterior IACs so that during seating the post or implant well is not distorted by tapping the IAC while its post is not properly aligned with the well of the implant because of interproximal contacts that are too tight.
- Incisal jig is only an initial guide for orientation.
- Aesthetics and occlusion should be the final determining factors for orientation.
- Interproximal contacts that are too tight can prevent proper orientation and engagement of the locking taper.
- While making extra-oral adjustments to the IAC, it is important to place a temporary abutment or healing abutment into the implant well to prevent soft tissue from closing the sulcus.
- A seating caliper alignment device facilitates and assures the fabrication of a seating jig with the proper alignment trajectory.
Page 1 | Page 2 | Page 3 | Page 4 | Page 5 | Page 6 | Page 7 | Page 8 | Page 9 | Page 10 | Page 11 | Page 12