Research Abstracts
- 3/17/16
-
Update on short, angulated and diameter-reduced implants
11th European Consensus Conference (EuCC) 2016 | Cologne, Germany | February 6, 2016
Jörg Neugebauer, PhD, DMD, Hans-Joachim Nickenig M.Sc., PhD, DMD, Joachim E. Zöller, PhD, MD, DMD, Director: Professor DDr Joachim E. Zöller
1. METHODS: 1.1 Objective:The purpose of these guidelines is to offer recommendations for clinicians engaging in implant dentistry, enabling them to correctly assess potential indications (and any limitations thereof) for short, angulated or diameter-reduced implants.
1.2 Introduction: This consensus paper covers only titanium implants typically placed in accordance with the indications recommended by the European Consensus Conference (EuCC, Germany, 6 February 2016). All consensus recommendations in this paper should be considered as guidelines only. The patient’s specific situation is always an important consideration and may justify a deviation from the recommendations of this consensus paper.
1.3 Background: Avoiding bone augmentation through reduced--dimension implants and optimum utilization of available bone volume is often recommended being a minimally invasive treatment option. To ensure an acceptable treatment outcome, dimension and insertion type must be considered in addition to the number of implants.
1.4 Literature search: The Cochrane Library, EMBASE, DIMDI and Medline literature databases were used to conduct a systematic search of recently published data on the use of short, angled or diameter-reduced implants. Selective search criteria were used, including terms such as “short implants”, “angulated implants”, “angled implants”, “tilted implants”, “outcome grafting procedure”, and “implant -failure”. The publications identified by the search were screened by reading their abstracts, and those irrelevant to the subject were identified and excluded. Publications found to be potentially relevant were obtained in full-text form. Multiple review papers with meta-analyses and randomized controlled trials (RCTs), and other prospective and retrospective systematic clinical studies were available on the subject.
1.5 Procedure for developing the Consensus Conference guidelines: A preliminary version of this document on which the EuCC based its deliberations was prepared by Dr J. Neugebauer of the Interdisciplinary Policlinic for Oral Surgery and Implantology and Department of Oral and Maxillofacial Plastic Surgery at the University of Cologne/Germany. The preliminary report was then reviewed and discussed by the sitting committee members in five steps as follows:
• Reviewing the preliminary draft
• Collecting alternative proposals
• Voting on recommendations and levels of recommendation
• Discussing non-consensual issues
• Final voting
The full text of all (potentially) relevant citations was obtained if necessary and reviewed. Numerous reviews, but few RCTs (randomised controlled trials) or other systematic clinical trials are available on this topic.
2. PROBLEM: The application of standard implants in patients with atrophy of their alveolar ridges or large pneumatization of the maxillary sinus cavity often requires the use of hard tissue augmentation procedures. These procedures are established, and widely used with success. But depending on level of training of the user and the patient-specific risk factors, complications may occur and affect the postoperative quality of life.
3. USE OF SHORT IMPLANTS: 3.1 Introduction: Short implants are increasingly being discussed as a treatment alternative in situations characterized by limited vertical bone height. Compared to the use of standard implants due to biomechanical considerations (e.g. crown-to--implant ratio, C/R) with short implants may lead to unfavourable loading conditions and complications, including excessive crestal bone loss and implant failure. Improvements in implant design and surface along with the use of modified implant insertion methods all are intended to minimize these risks
3.2 Definition of short implants: Implants are usually referred to as short if their designed intrabony length measures ≤ 8 mm with diameters ≥ 3.75 mm. Standard implants are considered to be those with lengths > 8 mm and diameters ≥ 3.75 mm. “Ultra-short” implants are considered to be those with lengths less than 6 mm.
3.3 Indications for short implants: Short implants are primarily used to avoid bone augmentation procedures in the maxillary and mandibular posterior segments of partially edentulous patients. They are applicable if vertical bone volume is limited by anatomical structures (maxillary sinus, mandibular canal), but there is sufficient alveolar ridge width to permit successful use of implant diameters ≥ 3.75 mm. They are also used to support removable overdentures as single or multiple tooth replacements in the anterior jaws.
3.4 Current observations: For ultra-short implants, there is insufficient evidence to make recommendations at this time. A review paper from 2015 summarized findings with RCTs on sinus floor elevation with standard length implants or short implants on their own. Five studies reported 16–18 months survival rates for long implants in combination with sinus elevation of 99.5 % (95 % CI: 97.6 – 99.98 %) and for short implants alone of 99.0 % (95 % CI: 96.4 – 99.8 %). For shorter observation periods of 8 – 9 months in three studies, survival rates for long implants were 100 % (95% CI: 97.1 – 100 %) and for short implants alone 98.2 % (95 % CI: 93.9 – 99.7 %). These results are supported by other RCTs.
The number of RCTs on the use in the mandible is limited. In these RCTs, no relevant differences in biological parameters between the use of short and long implants in the posterior mandible were found. One group has presented five-year results showing no significant difference for the application of short implants alone as compared to standard implants and vertical augmentation in the mandible.
A retrospective comparative analysis also showed no differences between short and long implants for an observation period of five years. Meta-analysis showed high survival rates for short implants with moderately rough surfaces. Long-term data for observation periods of 10 years for the posterior mandible of partially edentulous patients and 20 years for mandibular overdentures showed favourable results for short, sintered porous-surfaced implants.
The literature does show, however, that short implants with a reduced diameter have failure rates of up to 10 % after three to five years.
3.5 Prevention of complications: Some authors have offered recommendations on how to avoid complications that are mainly biomechanical in nature. These recommendations include:
• Machine-surfaced, short implants should not be used
• Short implants should only be used if bone -quality is favourable
• Restoration with single crowns
• Primary splinting of threaded short implants
• Guiding surfaces for lateral movements should be avoided
• Insertion at or below bone level with tapered abutment design
• The implant surgeon and restorative dentist should have adequate training
• For short implants no data available for immediate loading procedures
RECOMMNEDATIONS FOR SHORT, ANGULATED OR DIAMETER-REDUCED IMPLANTS: Provided the specific treatment parameters are observed, the use of short, angulated or diameter-reduced implants in sites with reduced bone volume can be a reliable treatment option, given the risks associated with the use of standard-dimension implants in combination with augmentation procedures. The implant surgeon and the restorative dentist must have appropriate training to choose the best possible therapy for each patient. Download PDF - 2/20/16
-
CAD/CAM Removable Bridge on Ultra-Short Implant in High Atrophic Maxilla
31st Annual Meeting of Academy of Osseointegration | San Diego, CA| February 17-20, 2016
Dr. Frank Kistler, Dr. Steffen Kistler; Stephan Adler, CDT; Priv.-Doz. Dr. Jörg Neugebauer
INTRODUCTION: The prosthetic treatment of the severe atrophic maxilla request quite often an implant placement after an intense grafting procedure. The acceptance of intense grafting procedures e.g. with hip graft or bilateral sinus graft is limited especially for elder patients with multiple general disease. The use of ultrashort implants is an option to avoid grafting procedures. Standard treatment of short implants is the performed with multiple single units or short span bridges. For edentulous jaws the resilient stabilization of cover dentures on ball attachments is recommended. The full-arch reconstruction with short implants is not documented in a routinely procedure for removable bridges.
MATERIAL and METHODS: In the last three years 12 patients with a severe atrophic maxilla were treated to receive a full arch reconstruction. 9 patients received six implants and 3 patients eight implants. All implants received a screw retained CAD/CAM milled bar after abutment placement. For a tension free delivery two impressions are necessary. First on implant level for the selection and preparation of the abutments. After the delivery of the abutment the final impression was performed.
RESULTS: All patients showed a compromised medical history with cardiovascular disease, stroke, COPD which did not allow an intense surgical procedure. 8 patients received the implant placement with local anesthesia and 4 patients with local anesthesia and medical monitoring. All patients showed no surgical complications and all implants showed osseointegration after three months healing period. After delivery of the prosthetic rehabilitation all patients were satisfied with the improved fixation of the superstructure. The speech function was not compromised due to the direct contact of the resin on the palate. The sensitivity for eating was improved because all superstructure worked without a coverage of the palate. Due to the severe atrophy a high restoration height was necessary with was between 16 and 28 mm. Due to the rigid fixation on the CAD/CAM milled bar no micro-movements occurred and the wear of the friction element was negligible.
CONCLUSION: Overall the placement of ultra-short implants in the high atrophic maxilla restored with a CAD/ CAM milled superstructure and a removable bridge is a complication free possibility to improve the quality of life on medical compromised elder patients. Download PDF - 12/01/15
-
Clinical and radiographic success rate of locking-taper implants placed on focal osteoporotic bone marrow defect patients. A longitudinal study
Clinical Oral Implants Research | December Vol. 26, Issue 12
M. Simancas, M. Marincola, G. Lombardo
BACKGROUND: Focal Osteoporotic Bone Marrow Defects (FOBMD) is described as a radiolucent area that is pathologically consistent with hematopoietic tissue in sites where an extraction has occurred. This disease is asymptomatic and it’s accidentally detected during radiographic analysis or any surgical procedure as dental implant placement. In a radiographic wise, it is localized, cortically demarcated that varies in size, shape and trabecular pattern. Having this in mind, the bone quality related with those areas can be poor which represents a challenging situation for clinicians on implant dentistry. FOBMD should be detected in the planning stages in order to avoid related complications as nerve damage, infection and implant displacement to a deep position that could represents also a prosthetic complication.
AIM/HYPOTHESIS: The aim of this observational retrospective longitudinal study is to describe the clinical and radiographic success rate of locking-taper implants placed on Focal Osteoporotic Bone Marrow Defects (FOBMD) patients in an area of Colombia, South America and its clinical implications for implant dentistry.
MATERIAL and METHODS: For this study we included 32 patients with FOBMD diagnosis. Patients were selected on the basis of a radiolucency presence in the posterior region of the jaws which was confirmed in the surgical implant placement. One trained oral surgeon placed 51 locking-taper implants (Bicon Dental Implants, Boston MA., USA) on these patients. On a small sam- ple of these 32 patients pathological samples were obtained and stored in a vial containing formaldehyde. Then pathological reports were obtained using haematoxylin-eosin technique by one experienced pathologist blinded to the clinical procedure and patient information. Additionally, a trained and calibrated dentist performed the clinical and radiographic evaluation of the patients. Clinical variables included implant-related complications. Radiographic outcomes comprised implant-surrounding radiolucency, implant displacement and bone loss. These radiographic examinations were performed using digital radiography with parallelism technique (Dr. Suni., Suni Medical Imaging., USA). Clinical and radiographic measurements were performed through a standardized questionnaire designed by the research team. Statistical analysis was performed through descriptive statistics for quantitative and qualitative data. Association between qualitative variables was obtained using Fisher’s exact test with a type I error degree of 0.05. All calculations were performed using the Stata v.13.1 for Windows statistical package (StataCorpTM., Texas., USA).
RESULTS: 22 of the patients were females for 68.7% of the sample with an overall age of 54.7 ± 11.8 years. The mean follow-up time after implant placement was 20.9 ± 8 months. It was placed one implant in 59.3% with a natural tooth as a neighbor in 35.2% and replacing a lower teeth in the 93.7% of the cases. The most frequent tooth extraction reason was previous endodontic treatment/infection in 82.3% (CI 95%:68.8–90.7) of the cases, additionally the mean time since the extraction was 117.9 ± 91.3 months. Pain and implant displacement occurrence were 3.9% (CI 95%: 0.93–14.9). Other findings were bone loss and implant placed in proximity with a natural tooth. Histological findings showed calcification areas surrounded by hemor- rhage, dystrophy and inflammatory cells in the samples. One implant was considered as failure due to fiber-integration. Thus, the overall success rate was 98% (CI 95%: 86.5–99.7). Neither the demographic or clinical parameters were associated with implant failure (P > 0.05)
CONCLUSION: FOMBD is a frequent pathology that should be detected in early stages of the implant treatment. Its presence is highly related with previous extractions and endodontic treatment sites and its treatment must be performed having in mind the extension of the lesion, some cases could be treated in conjunction with bone graft in order to maximize the implant stability. Nevertheless our results show that a high survival rate can be achieved considering the ade- quate treatment planning for the patients. Download PDF - 12/01/15
-
Post-extractive and delayed implant placement in aesthetic areas using locking-taper implants: a 3-year comparative study
Clinical Oral Implants Research | December Vol. 26, Issue 12
J. Pighi, G. Lombardo, G. Corrocher, M. Simancas Pallares, M. Marincola, P. Nocini1
BACKGROUND: Implant therapy in partially edentulous patients has become a well-established treatment method even in aesthetic areas, where predictability levels comparable with those for implants placed in other jaw areas have been achieved. To shorten rehabilitation times, protocols have been constantly evolving in recent decades, with the literature focussing on the evaluation of post-extractive implant placement with or without immediate loading. Now these protocols achieve implant survival rates comparable to those of traditional biphasic techniques, thanks to continuous improvements of materials and methods. Most of the studies have focused on implant survival, however in aesthetic areas complications such abutment or implant collar expo- sure, or the absence of interproximal papilla, may have serious implications even if good osseointegration has been reached. There have been in literature few studies employing indices that can be objectively re-used for comparative aesthetic appraisal.
AIM/HYPOTHESIS: The purpose of this study was to compare the aesthetic outcome and the stability of peri-implant hard and soft tissues of single-tooth locking-taper connection implants placed in the anterior maxilla in fresh or healed post-extractive sock- ets.
MATERIAL and METHODS: Twenty-one patients received 34 plateau design locking-taper implants (Bicon LLC, Boston, MA, USA) in the anterior maxilla. Fourteen implants were placed immediately after tooth extraction, whereas 20 implants were placed after the healing of alveolar socket. The presence of teeth or implants as mesial and distal adjacent was evaluated. To objectively examine the aesthetic outcome of the implants, intraoral photographs were critically analysed using the Papilla Index. Moreover, the health condition of peri-implant soft tissues such as probing depth (PD), modified bleeding index (mBI), modified plaque index (mPI) and width of keratinized mucosa (KT) were evaluated. In relation to peri-implant hard tissues, the interproximal bone peaks (crestal bone, CB) and the first bone-to-implant contact (FBIC) were measured on mesial and distal sides using a soft- ware program (Rasband, W.S., ImageJ, U. S. National Institutes of Health, Bethesda, Maryland, USA). Student T test was used to study the differences between post-extractive and delayed implants regarding the study variables, and to find any differences regarding sites with a tooth or an implant as adjacent. The significance was set to P < .05. Results: The average follow-up period was 38.6 ± 24.1 months. No implants or prostheses were lost (CSR = 100%). Most of the patients exhibited good oral hygiene during the follow-up period, presenting with a plaque index (mPI) of 0.13 ± 0.32 and a bleeding index (mBI) of 0.19 ± 0.18. The average probing depth (PD) was 2.64 ± 0.57 mm. The average amount of peri-implant keratinized tissue (TK) was 3.84 ± 1.35 mm. Differences were only found regarding the width of keratinized mucosa (post-ex: 4.57 ± 1.64 mm; delayed: 3.33 ± 0.86 mm; P = 0.007). The average CB level was 2.38 ± 1.65 mm (post-ex: 2.53 ± 0.91 mm; delayed: 2.28 ± 2.03 mm; P = 0.67). The average FBIC was 0.26 ± 0.39 mm (post-ex: 0.21 ± 0.06 mm; delayed: 0.33 ± 0.47 mm; P = 0.17). The mean Papilla Index was 1.84 ± 0.78 (post-ex: 2.25 ± 0.78; delayed: 1.55 ± 0.65; P = 0.01). The average papilla score was 1.98 ± 0.71 when there was a tooth as adjacent, and it was 1.61 ± 1.02 when there was an implant as adjacent (P = 0.09).
CONCLUSION: The rehabilitation of both function and aesthetics at the same time as tooth extraction, using a post-extractive immediate non-functional loading protocol, is a major challenge for the therapist but offers great benefits for the patient. Within the limits of this study, single-tooth Morse taper connection implants placed in the anterior maxilla according to an immediate non-functional loading protocol seems to be comparable to delayed implant placement for the main- tenance of peri-implant hard and soft tissues, and even better from an aesthetic point of view. Download PDF - 3/6/14
-
Short Dental Implants: A Reality for Complex Cases
29th Annual Meeting of Academy of Osseointegration | Seattle, WA| March 6-8 2014
Rodrigo Kaiser DDS, Eduardo Varas DDS, Cristina Antunez DDS
Facultad de Odontología, Universidad Finis Terrae, Chile
ABSTRACT: PURPOSE:To evaluate the performance of short implants.
MATERIALS AND METHODS: A retrospective cohort study was conducted between October 2009 and August 2013. The sample was composed of patients who had received at least one short implants, Bicon implant.
RESULTS: Forty subjects who received 124 implants were followed for an average of 47 months. One hundred five implants (84.68%) were restored with single crowns. Three implants failed, for a cumulative survival rate of 97.58%. Of the failed implants, all were of 5 x 6.0mm.
CONCLUSIONS: The survival of short implants was comparable with normal implants.
INTRODUCTION: Implant therapy based on the principle of implant osseointegration has been very well documented and is accepted widely. However, the placement of long dental implants in some anatomic sites, such as the posterior maxilla and mandible, may be limited by the residual ridge height.
CONCLUSION: This research reports the 4-year clinical experience with short dental implants in Chile. Survival rates of 97.58% were obtained for the short implants, the majority of which were restored with single implants restoration (84.68%) These results demonstrated the predictability and biosafety of these short implants when used with careful treatment planning and a strict clinical protocol. Download PDF - 3/21/13
-
Composites For Implant-Supported 3-Unit Fixed Dental Prostheses: Reliability and Fractography
IARD | Seattle, WA| March 21, 2013
Bonfante, E., Postgraduate Program in Dentistry, UNIGRANRIO University, Bauru, Brazil, R.M. CARVALHO, Oral Biological and Medical Sciences, University of British Columbia, Vancouver, BC, Canada, M. SUZUKI, Tufts University, Boston, MA, N.R. SILVA, Federal University of Minas Gerais UFMG, belo Horizonte, W. LUBELSKI, Dental Implant Center, Boston, MA, L. WITEK, School of Chemical Engineering, Oklahoma State University, Stillwater, OK, and P.G. COELHO, Biomaterials and Biomimetics, New York University, New York, NY
OBJECTIVES: To evaluate the reliability and failure modes of 3-unit implant-supported fixed-dental-prostheses (FDP) made of an indirect composite veneered onto a CAD/CAM fiber-reinforced-composite framework (FRC) or used as a monolithic prosthesis (ML), and compare to metal ceramic (MC).
METHODS: Twenty-one indirect composite 3-unit posterior FDP (Ceramage, Shofu, Japan) were incrementally veneered directly onto two titanium abutments (Stealth abutment, Bicon, USA) (ML group) simulating the loss of the first mandibular molar. A composite FDP was scanned and 21 FRC-frameworks (Trinia, Bicon, USA) were milled and layered with the same indirect-composite to obtain the same anatomy of the ML. FRC FDP were cemented (RelyX-U100, 3M-ESPE) and all FDP-abutment assemblies were connected to implants (n=126, Bicon, USA) and embedded in acrylic resin. Twenty-one PdAg-MC FDPs were tested for comparison. Samples were subjected to single-load-to- fracture (SLF, n=3 each) for determination of step-stress profiles for accelerated-life fatigue-testing in water (n=18 each). Beta-values were calculated and Weibull curves with use-stress of 300 N for a mission of 100,000 cycles (90% CI) plotted.
RESULTS: Mean SLF was 812 N for ML, 968 N for FRC, and 945 N for MC. Beta values were 0.41 for ML, 0.5 for FRC, and 0.55 for MC indicating that strength was the main factor dictating failure of groups. The data replotted as Weibull distribution showed an m=5.81 and η=742.72 N for ML, m=6.75 and η=643.59 N for FRC, and m=3.82 and η=682.11 N for MC (p>0.1). Reliability for a mission of 100,000 cycles, 300 N was 98% for ML, 96% for FRC, and 88% for MC (p>0.1). Fatigue fracture was catastrophic for ML, cohesive within the resin or exposing the FRC framework, and cohesive within the porcelain/exposing the framework of MC.
CONCLUSION: Reliability was not significantly different between groups. Failure modes were different.
SUPPORT: APESP grant # 2010/06152-9 and Bicon Implants.
- 3/22/13
-
Sandblasting improves bonding of resin-composite to CAD/CAM fiber reinforced composite
IARD | Seattle, WA| March 22, 2013
Vidotti, H. A.
Prosthodontics, University of Sao Paulo, Bauru-SP, Brazil, R.M. CARVALHO, The University of British Columbia, Vancouver, BC, Canada, N.R. SILVA, Federal University of Minas Gerais UFMG, belo Horizonte, A.L. VALLE, Prosthodontics, University of São Paulo, Bauru SP, Brazil, P.G. COELHO, Biomaterials and Biomimetics, New York University, New York, NY, and E.A. BONFANTE, Postgraduate Program in Dentistry, UNIGRANRIO University, Bauru, Brazil
OBJECTIVES: This study investigated the effect of sandblasting on the bond strength of an indirect resin composite veneered to a CAD/CAM fiber reinforced composite framework material.
METHODS: Ten CAD/CAM fiber reinforced composite blocks (Trinia, Bicon, Boston, USA) were polished to a 600-grit silicon carbide paper. Half of the specimens (n=5) were sandblasted (SB group) with 50 μm Al2O3 particles. The other 5 samples were not sandblasted (No-SB) and only subjected to adhesive system bonding treatment. All blocks were cleaned in an ultrasonic bath before bonding procedures. A two-step adhesive system (CRB, Shofu Dental Corporation, Kyoto, Japan) was applied, 10 seconds allowed for solvent evaporation for each step, and then light-cured for 10 seconds. An indirect resin-composite (Ceramage, Shofu Dental Corporation, Kyoto, Japan) was incrementally packed (1,5 mm) and light-cured for 60 seconds. The layered blocks were longitudinally sectioned with a diamond saw under water irrigation. Forty- five stick-shaped samples with an approximate 1mm2 cross-section area were obtained for each group and tested in a microtensile mode at 0,5 mm/min. Fracture analysis was performed by optical and scanning electron microscopy. Only data from interfacially failed specimens were included on statistical analysis. Weibull Distribution Analysis (95% confidence bounds) was used to determine and to plot characteristic strength (Eta in MPa) and the Weibull modulus (m) for each group.
RESULTS: The sandblasted group (SB) showed higher Eta (41.94 MPa) and m (12.55), compared to the group without sandblasting (No-SB) (Eta=36.9 MPa, m=6.98).
CONCLUSION: Both groups showed high values of bond strength. However, sandblasting significantly improved the bonding between the materials tested and provided less variability of the bonding results as shown by the higher Weibull modulus obtained.
- 10/5/12
-
The Correlation Between the Nonsteroidal Anti-Inflammatory Drugs and the Changes in Crestal Bone Levels Surrounding Dental Implants
AAID | Washington, DC | Oct. 5, 2012
Dragan, I.F.
Periodontology Department, Tufts University School of Dental Medicine
INTRODUCTION: Nonsteroidal anti-inflammatory drugs (NSAIDs) are the most prescribed analgesics for the treatment of dental pain. The current literature provides data regarding the effect of NSAIDs on the alveolar bone metabolism. Minimal bone loss is considered an indicator of the success of dental implants.
SUMMARY: The aim of this study was to conduct a literature review and identify the manuscripts that report a correlation between peri-implant bone levels and NSAIDs.
MATERIALS AND METHODS: An electronic search of MEDLINE (PubMed) database was conducted using the following criteria: “(nonsteroidal anti-inflammatory drugs)” AND “dental implant”. All the manuscripts included in the study pertain to human studies and mention the follow-up period of the subjects.
RESULTS: Initial screening was performed using the titles and the abstracts resulted from the searching process. A number of 59 papers were identified, but only five of them were eligible to be included in the review. The study designs analyzed were: randomized controlled clinical trial, meta-analysis and retrospective cohort.
CONCLUSION: Beneficial effects of the NSAIDs for the crestal bone levels surrounding dental implants have been reported. Several manuscripts reported on a significant reduced peri-implant bone levels on patients treated with NSAIDs, but only one of the manuscripts reported a crestal bone gain. The data available is sparse and more studies need to be conducted in order to establish a relevant correlation. Further criteria that evaluate a successful dental implant should be considered.
- 10/2/12
-
Comparison of Crestal Bone Level Changes Surrounding Five, Six, and Eight Millimeter Long Platform-Switching Implants
AAP | Los Angeles, CA | Sept. 29-Oct. 2, 2012
Dragan, I.F. • Chuang, S.K. • McKenna, M. • Urdaneta R.A.
Periodontology Department, Tufts University School of Dental Medicine
MD Oral and Maxillofacial Surgery Department, Harvard School of Dental Medicine and Massachusetts General Hospital
The Implant Dentistry Centre
BACKGROUND: Short implants are an alternative to bone grafting procedures followed by implant placement for the treatment of posterior edentulous areas with limited bone height. The clinical performance of five and six millimeters long implants requires further study. The purpose of the present investigation was to evaluate the crestal bone levels surrounding five millimeters wide platform-switching implants with three different lengths (five, six and eight millimeters).
METHODS: The study design is a retrospective cohort study - the population of patients included had at least one five millimeters wide implant with eight millimeters length or less. For the purpose of this study, implants eight millimeters in length were defined as “short” and five and six millimeters long implants were defined as “ultrashort”. Descriptive statistics, univariate, and multivariate generalized linear mixed models and Cox proportional hazard regression models, adjusted for multiple implants in the same patient were utilized to evaluate the effect of length in changes of crestal bone levels (AvCBL) surrounding five millimeters wide platform-switch implants.
RESULTS: A total of 369 implants were followed for an average period of 42 months. The cohort consisted of 197 ultrashort implants, 172 short implants and documented 10 failures: six from the ultrashort group and four from the short group. It was reported an AvCBL of 0.07 mm and 0.15 mm for ultrashort and short implants respectively. The multivariate analysis revealed that implant length was not a significant risk factor for peri-implant bone for five millimeters wide implants (p=0.85). The study suggests that immediate loading, daily intake of nonsteroidal anti- inflammatory drugs (NSAIDs) and bone augmentation procedures with beta-tricalcium phosphate are associated with a significant increase in crestal bone levels for this particular cohort. On the other hand, the removal of the adjacent tooth structure was associated with peri-implant bone loss for the same considered group.
CONCLUSION: Platform-switching five millimeters wide implants with five, six and eight millimeters length demonstrated similar crestal bone level stability. The clinical significance of these findings is that five and six millimeters long implants may be used to restore edentulous areas with limited bone height. Download PDF - 07/14/10
-
Reliability of Abutments Veneered with Indirect Composite for Implant-Supported Crowns
IADR | Barcelona, Spain | July, 2010
Bonfante, EA • Suzuki, M • Lubelski, W • Silva, NR • Coelho, PG
University of São Paulo, Bauru School of Dentistry, Brazil
Tufts University School of Dental Medicine, USA
Bicon Dental Implant Center, USA
New York University, Biomaterials and Biomimetics, USA
OBJECTIVES: To investigate the reliability/failure modes of different supporting size abutments veneered with indirect composites for implant-supported crowns.
MATERIALS AND METHODS: Regular size abutments (R) (6.35 mm diameter base, with a 4 mm high and 2 mm diameter post in the center for composite retention), small (S) (5.2 mm base, 4 mm high and 2 mm diameter post), and small with post shortened (SS) to 2 mm height titanium abutments (Fig. 1) (Bicon LLC, Boston, USA,) received incremental layers of indirect resin composite (Ceramage, Shofu, Japan) until complete the anatomy of a molar crown (Fig. 2). Three crowns of each material were loaded until failure for determination of stepstress profiles for accelerated-life fatigue testing (n=18 each). Weibull curves with use-stress of 200N for 50K cycles (90% confidence intervals) were calculated and plotted using a power law relationship for damage accumulation. Weibull modulus "Beta" and characteristic strength "Eta" were identified and a contour plot was used (Beta vs. Eta) for examining differences between groups. Specimens were inspected in light and scanning electron microscope.
RESULTS: Beta values were 0.27 for R, 0.25 for S, and 0.26 for SS abutments, indicating that failures were not influenced by fatigue and damage accumulation, whereas strength was the main factor dictating failure of groups (Fig. 3). The data was replotted as Weibull distribution and the characteristic strengths of 796 N and 832 N for R and S abutments, respectively, were not significantly different (confidence bounds overlap, p > .10), but significantly higher than 588 N for SS (Fig. 4). Reliability data is presented in Table 1. Failure mode was cohesive within the composite for R and S, and mixed cohesive and crown debond from abutment for SS (Fig. 5).
CONCLUSION: Reliability for a mission of 50 K cycles at 200 N was not significantly different between different abutment designs. Failure modes differed. Download PDF - 05/01/10
-
Implant Survival Rates and Endodontic Treatment
CDA 2010 Meeting | Anaheim, CA | May, 2010
Sooyoung Kim • Kim M. Emanuel • Sung-Kiang Chuang
Department of Mechanical amd Industrial Engineering, Northeastern University
UCSF School of Dentistry, San Francisco, CA
Implant Dentistry Centre, Boston, MA
Massachusetts General Hospital – Harvard School of Dental Medicine, Boston, MA
ABSTRACT: In this retrospective cohort study, implant survival rates at or adjacent to sites with previous root canal treatment (RCT) were studied. The sample was composed of 619 implants (placed from 2001 to 2007) and categorized into three groups. Group 1 was composed of implants placed at sites with RCT history. Group 2 included implants placed adjacent to tooth/teeth with RCT on either/both sides. Group 3 was a control which did not meet the above conditions. Appropriate descriptive, Kaplan-Meier (K-M) survival analysis was computed to obtain and compare 1-year survival rates of these three groups. The 1-year survival rates for Group 1, Group 2, and Group 3 were 95.9%, 97.4%, and 99.1%, respectively. The control group had the highest survival rate at 1 year when compared with Group 1 or 2. However, all three groups are consistent with reported successful 1-year survival rates over 90%.
MATERIALS AND METHODS: A retrospective cohort study was conducted in order to assess impact of previous endodontic treatment on implant survival rates. The cohort was composed of patients having implants placed from July 1, 2001 to December 31, 2007 at the Implant Dentistry Centre in Boston.
RESULTS: These results are consistent with other studies, which used the same type of implants used in this study. In those studies, 1-year survival rates ranged from 93.9 – 95.2% [10, 11].
CONCLUSION: The 1-year survival rates for Group 1, Group 2, and Group 3 were 95.9%, 97.4%, and 99.1%, respectively. The control group had the highest survival rate at 1 year when compared with Group 1 or 2. However, all three groups are consistent with reported successful 1-year survival rates over 90%. A more rigorous statistical analysis will be performed on the dataset to test for significance. Download PDF - 05/01/10
-
Biomechanical and bone histomorphologic evaluation of four surfaces on plateau root form implants: An experimental study in dogs
AADR 2010 Meeting | Washington, DC | March, 2010
Coelho, P.G. • Granato, R. • Marin, C. • Bonfante, E.A. • Janal, M.N. • Sukuki, M.,
Assistant Professor, Department of Biomaterials and Biomimetics, New York University, New York, New York
OBJECTIVE: To evaluate the early bone response to plateau root form dental implants with 4 different surface treatments.
STUDY DESIGN: Surface treatments comprised (n=12 each): as-machines (M), alumina-blasted/acid-etched (AB/AE), alumina-blasted/acid-etched + nanothickness bioceramic coating (Nano), and plasma-sprayed calcium phosphate (PSCaP). Implants were placed in the radius diaphyses of 12 beagle dogs, remaining vivo for 3 and 5 weeks. After euthanasia, the implants were subjected to torque to interface fracture and subsequently nondecalcified for histomorphology. Statistical analysis was performed by GLM analysis of variance model at 5% significant level.
RESULTS: Torque to interface fracture was significantly greater for the PSCaP group than for other groups (P < .001). Histomorphologic analysis showed woven bone formation around all implant surfaces at 3 weeks, and its replacement by lamellar bone at 5 weeks. Time in vivo did not affect torque measures.
CONCLUSIONS: The PSCaP surface increased the early bone biomechanical fixation of plateau root form implants. - 03/06/10
-
Bone Remodeling Due to Dental Implants by Finite Element Analysis
AADR 2010 Meeting | Washington, DC | March, 2010
Hsuan-Yu Chou • Sinan Müftü
Department of Mechanical & Industrial Engineering, Northeastern University
BACKGROUND: The aim of this study is to predict the adaptation of bone density to mechanical stimuli following dental implantation by using a mathematical bone remodeling algorithm and the finite element method.
MATERIAL AND METHODS: The bone remodeling algorithm developed for long bone was adopted in this study, where the change or lack thereof of the bone density depends on the difference between the attractor and current bone stimuli. In this study, a representative bone volume, where the trabecular bone is surrounded by a layer of cortical bone, was constructed from a mandibular CT scan. The effects of the natural tooth and various implant systems in its place were investigated. In particular, the attractor stimulus is based on the loading of the bone with an intact natural tooth. This attractor stimulus is then used for the bone remodeling predictions for the cases with dental implants. All materials were assumed to be linear, elastic, homogeneous and isotropic. Occlusion was simulated by applying an oblique load of 100N on the crown.
RESULTS: Significant bone remodeling, which causes inhomogeneous distribution of bone elastic modulus, was predicted in the region close to the bone implant interface. The amount of remodeling decreases away from the implant surface, and as a result, material properties of the bone distal to implant remain unchanged.
CONCLUSIONS: It is expected that biomechanics of bone is altered as a result of the geometric and material differences between a natural tooth and a dental implant. This study demonstrates such biomechanical alteration can lead to the bone remodeling, and which can influence the long term stability of dental implant. The bone remodeling predictions can be useful in designing implant contours with the goal of long term implant survivability. This study is supported in part by Bicon Dental Implants. Download PDF - 09/07/08
-
Sinus Augmentation Procedure Using Beta-Tricalcium-Phosphate: Histological Analysis of Grafted Bone at Time of Implant Placement
American Academy of Periodontology 94th Annual Meeting & Exhibition | Seattle, WA | September, 2008
Ulrike Schulze-Späte1, Thomas Dietrich1, 2, Justine Dobeck3, Rayyan Kayal1, Adrian Time1, Ziedonis Skobe3, Serge Dibart1
1Department of Periodontology and Oral Biology, Goldman School of Dental Medicine, Boston University, Boston, MA,
2University of Birmingham, UK
3The Forsyth Institute, Boston, MA
BACKGROUND: Implant placement in the edentulous maxilla often represents a clinical challenge due to insufficient bone height after crestal bone resorption. Several graft materials have been evaluated for augmenting the maxillary sinus in order to compensate for the lost vertical dimension. Allografts are readily available, there is no risk of disease transmission and they do not require a second site surgery.The aim of this study was to evaluate the development and maturation of augmented bone in the maxillary sinus using beta-tricalcium phosphate.
MATERIAL AND METHODS: Patients (n=10, female: 4/male 6, age 30-64) with the need for rehabilitation of their dentition in the posterior maxilla and no present medical contraindications were included in the study. Beta-tricalcium phosphate (SynthoGraft, Bicon, Boston, MA) mixed with the patient’s blood was implanted into the sinus cavity, which was accessed using a lateral window technique. 6-8 month post sinus elevation, bone biopsies were taken and implants were placed simultaneously. All specimens were demineralized and subjected to staining procedures (H&E, Goldner's staining, TRAP). Slides were analyzed using lightmicroscopy for total surface area, the surface area that consisted of bone and the surface area that consisted of graft material (all in mm2 and expressed as % of the total surface.). Osteoclasts were identifiedand counted as number per mm2.
RESULTS: All implants were placed achieving primary stability and restored 4 months after placement. H&E and Goldner's stainings demonstrated the presence of vital woven bone in the grafted area withonly a few remaining graft particles (total bone surface: 31.3%±15.8% at 6 month and 36.4%±5.4% at 8 month, total graft surface:13.9%± 4.7%at 6 month and 9.6%±4.8%). In addition, TRAP staining revealed presence of osteoclasts surrounding those particles (osteoclast number:1.23±0.25 per mm2 at 6 month and 1.4±0.4 per mm2 at 8 month). A lack of inflammatory reaction was noticed with the use of this graft material. During 12 month follow up, no implant failure or complications were observed.
CONCLUSIONS: Beta-tricalcium-phosphate has the advantage of exhibiting no risks of disease transmission and can be available in unlimited quantities. It is clinically easy to use, having great handling properties and appears to cause no persistent inflammatory reaction insurrounding bone. Overall this material seems to provide adequate stability at time of implant placement. Therefore, augmentation of the maxillary sinus with beta-tricalciumphosphate represents a viable option for increasing vertical bone height in the posterior maxilla prior to implant placement. Download PDF - 02/28/08
-
Crown-Implant Ratios of 6mm Length Implants
Academy of Osseointegration 2008 Annual Meeting | Boston, MA | February, 2008
Hardeep (Bobby) Birdi, DMD • John Schulte, DDS, MSD • Alejandro Rodriguez-Kovacs, DDS • Meghan Weed, RDH • Sung-Kiang Chuang, DMD, MD
University of Minnesota School of Dentistry
INTRODUCTION: Unfavorable crown-implant ratios have not yet been established. Still, excessive crown-implant ratios have been cited in the literature as being detrimental to long term implant success. The primary aim of this study was to determine the crownimplant ratios of single implant-supported fixed restorations on 6mm length implants in a clinical practice, and to evaluate the health of these implants via mesial and distal bone levels. Additionally, the relationship between crown-implant ratio and proximal bone levels was to be evaluated.
MATERIAL AND METHODS: In this retrospective cohort study the cohort was composed of 314 patients possessing at least one single 6mm length plateau design implant supported fixed restoration which had been surgically placed between Feb 1997 and Dec 2005. A chart review was performed to acquire radiographs in which both the entire crown and implant were visible. The length of the crown and implant were measured directly from the radiographs using consistent magnification to calculate the crown-implant ratio. Also, the mesial and distal bone levels were measured using 3 times magnification and mathematically corrected for distortion. The last available radiograph was used to measure bone levels. Follow-up time was calculated from the day of implant placement, to the last available radiograph. Statistical analyses using analysis of variance mixed models were used.
RESULTS: Data from 534 single implant supported fixed restorations were tabulated and included in the study. The mean (SD) follow-up time was 15.8 (19.2) months, with a range of 0.01 to 99.2 months. The mean crown length (SD) was 13.3 (2.7) mm, with a range of 2.4 to 21.7 mm. The mean (SD) crown-implant ratio was 1.97 (0.4) and ranged from 0.36 to 3.2. The average mesial and distal bone levels (SD) measured from the final radiographs were -0.2 (0.7) mm and -0.2 (0.9) mm respectively. There was no statistically significant relationship between increasing crown-implant ratios and decreasing mesial and distal crestal bone levels around the implant with p-values of 0.94 and 0.57 respectively.
CONCLUSIONS: The results of this study suggest crown-implant ratios do not affect long term success of 6mm length implants. Also, there are no associations between crown-implant ratio and crestal bone levels. Download PDF - 02/28/08
-
Preliminary Results of the Survival of 5 x 6 mm Implants
Academy of Osseointegration 2008 Annual Meeting | Boston, MA | February, 2008
Augusto Saldarriaga, DDS • Michael R. Markiewicz, BS • John Schulte, DDS, MDS • Meghan Weed, RDH • Sung-Kiang Chuang, DMD, MD
University of Minnesota School of Dentistry
INTRODUCTION: Manufacturers of dental implants have introduced short implants for use in areas of vertical alveolar bone deficiency. The literature regarding the survival of short implants is mixed. Recent modifications in the geometric shape and surface treatments of short implants may contribute to a rate of survival comparable to their longer counterparts. The objective of this study was to determine the short term survival of a 5 x 6 mm plateau designed dental implant.
METHODS: A retrospective cohort study design was used. The cohort consisted of patients who received one or more 5 x 6 mm plateau designed implant inserted between January 2005 and August 2006 at a private practice clinic. A chart review was conducted to acquire data on patient demographics, implant location, bone density, length of time in function and/or implant failure. The primary outcome variable was implant failure. Survival time was defined as the time between the date of implant placement and last appointment or the date of implant removal for any reason. Descriptive statistics are reported.
RESULTS: The sample included 542 implants placed in 324 patients (52.8% female). Mean patient age was 56.6 + 13.1 years. All 5 x 6 mm plateau designed implants were placed using a two stage technique. 301 (56%) implants were placed in bone density three and 151 (28%) implants in bone density four. 226 (41%) were placed in the posterior maxilla and 265 (49%) in the posterior mandible. The average follow-up time the implants were in function was 13.3 + 8.4 months, range 0.1 to 30.4 months. 35 failures were recorded for a survival rate of 92.1%. 20 (57%) of the failed implants were placed in type three bone density and 13 (37%) in type four density bone. 17 (49%) of the failures were in the posterior maxilla and 11 (31%) in the posterior mandible.
CONCLUSION: The short term survival of the 5 x 6 mm plateau designed implant is encouraging. Additional observation time is necessary to establish long term survival rates. Download PDF - 02/28/08
-
Crestal Bone Level and its Association With Varying Densities of Bone
Academy of Osseointegration 2008 Annual Meeting | Boston, MA | February, 2008
Sujey Rodriguez-Lozano, DDS • John Schulte, DDS, MDS • Meghan Weed, RDH • Sung-Kiang Chuang, DMD, MD
Graduate Prosthodontics, University of Minnesota School of Dentistry
INTRODUCTION: Crestal bone levels associated with dental implants are an indication of the health or status of the implant.
PURPOSE: The purpose of this study was to evaluate crestal bone levels on plateau designed implants in various densities of bone.
METHODS: A case series study design was used. The sample was composed of patients who had single tooth implant supported restorations placed between February 1997 and August 2006 with densities of bone information available in the charts. Bone levels on the mesial and distal surfaces of the implants were established by direct measurement from the top of the implant to the radiographic position of the bone on the implant surface. Radiographs were mathematically corrected for distortion. Bone density was determined objectively by examination of the bone which collected on the flute of the reamer during preparation of the osteotomy. Type I bone was characterized by bone which had minimal blood content, type II bone by blood wetted bone in the reamer, type III bone by a partially filled reamer of blood wetted bone and type IV bone as a reamer devoid of bone. Descriptive statistics were computed and data was analyzed with analysis of variance mixed models.
RESULTS: The sample consisted of 214 patients (50.0% females), Average age of the patients was 56.6 years. 264 plateau designed implants were included in this study. 50 implants were placed in type II bone density, 117 implants were placed in type III bone density and 97 were placed in type bone IV bone density. The mean age of implants was 2.3 ± .8 years. Mesial and distal bone levels in each of the 4 types of densities was reported as: For density type II: mesial -.9 ± .6 mm and distal -.9 ± .6 mm. For density type III: mesial -.8 ± .7 mm and distal -.8 ± .9 mm. For density type IV: mesial -.8 ± .6 mm and distal -.8 ± .5 mm. Statistical testing reveals no statistically significant differences in mesial bone levels (P=0.38) and distal bone levels (P=0.79) between the three groups of bone densities.
CONCLUSIONS: This study suggests that the crestal bone loss associated with the plateau designed implant is well within guidelines established in the literature. Secondly, there is no statistically significant difference in the crestal bone levels when comparing various densities of bone. The results of the study are relevant only to the plateau design implant. Download PDF - 02/28/08
-
In Vivo Evaluation of Implant Length and Surface Physico/Chemistry Characteristics in Biomechanical Anchorage in Plateau Root Form Implants. An Experimental Study in Beagle Dogs.
Academy of Osseointegration 2008 Annual Meeting | Boston, MA | February, 2008
Granato R, Marin C, Suzuki M, Gil JN, Coelho PG
Introduction: Since the implant surface is the first part of the implant that interacts with the host, significant attention has been devoted towards increasing the biocompatibility and osseoconductivity of implant surfaces. Surface modification approaches have been successful in increasing the host response to surgical implants, resulting in higher bone-to-implant contact (BIC) and higher bone mechanical properties at early implantation times. Among surface chemistry modifications, the incorporation of Ca- and P-based bioceramic onto the implant surfaces through various manufacturing processes has been investigated throughout the last two decades. These basic and clinical investigations have shown that bioceramic coated implants presented higher degrees of osseoconductivity and attained higher degrees of biomechanical fixation at earlier implantation times compared to uncoated implants. The objective of this study was to determine the influence of implant length and surface chemistry (Alumina-blasted/acid-etched (AB/AE) vs. Nanotite (Na) bioceramic deposition) on the biomechanical fixation of plateu root form implants in a beagle dog tibia model.
Methods: 4.5x11 mm (L) and 4.5x6 mm (S) plateau root form implants of AB/AE and Na surfaces were placed bilaterally along the proximal tibia of 6 beagle dogs and remained for 2 and 4 weeks in vivo (n=9 per implant length, surface, and time in vivo).(Fig. 1 and 2) Following euthanization, the implants were torqued to interface failure at ~0.445 radians/sec.(Fig. 3 and 4) ANOVA was utilized to determine the effects of implant length, surface, and time in vivo as (independent variables) on torque to interface failure (dependent variable). One-wayANOVAwas utilized for direct comparison between groups.A95% level of significance was used.
Results: trans-surgical bone preparation showed that L implants engaged two bone corticals whereas S implants engaged one cortical. ANOVA showed that all independent variables presented a significant effect in torque to interface (Ncm) failure: Implant length (P<0.0005, S=43.75±11.02 , L=72.02±10.54 ), implant surface (P<0.0000, AB/AE=34.93±10.85 , Na=80.84±10.7 ), and time in vivo (P<0.002, 2W= 45.51±10.7 , 4W=70.27±10.85 ). One-way ANOVA showed significant differences between groups (P<0.0000, seeTable 01).
Conclusions: According to the results obtained, the Nanothickness bioceramic surface coating played a significant role on biomechanical fixation of L and S implants at both times in vivo. While ANOVA showed a significant effect of implant length on biomechanical fixation, direct comparison between groups showed that this difference was larger for Nanotite coated implants, and not significantly different for uncoated implants. Download PDF - 02/28/08
-
A Comparison of Crestal Bone Levels in Immediate Versus Delayed Loaded Implants
Academy of Osseointegration 2008 Annual Meeting | Boston, MA | February, 2008
Cary D. McNeil, DDS ■ John K. Schulte, DDS, MSD ■ Meghan Weed, RDH ■ Sung-Kiang Chuang, DMD, MD
University of Minnesota School of Dentistry
INTRODUCTION: The results of implant survival studies as they relate to immediate versus delayed loading are inconclusive. Some report greater failure rates with immediate loading and others show no difference between the two procedures. Implant failure is often associated with excessive bone loss over time. As a result, bone loss over time may be a critical measurement of implant health. The objective of this study was to determine if there were differences in crestal bone levels over time with immediately loaded plateau design implants compared with delayed loaded plateau design implants.
METHODS: A retrospective cohort study was used. The cohort consisted of patients who received a single tooth plateau designed implant, immediate or delayed loading, between January 1997 and July 2005. Digital radiographs were retrieved from patient records. Mesial and distal bone levels were measured directly on the radiographs using 3x magnification and mathematically corrected for distortion. Changes in bone levels over time were calculated by comparing levels at post-integration with the last available film. Analysis of variance mixed models adjusted for clustered effects was used to test for statistical significance between the two groups.
RESULTS: A total of 483 implants were included in this study. The initial radiographic measurement of bone levels was set at 10 months after implant placement and was followed with a mean follow-up time of 19.3 months. The mean patient age was 55.3 years and 48.9% were female. There were 204 implants which were immediately loaded and 278 implants which were delayed loaded. Mean changes in mesial and distal bone levels for the immediately loaded implants were 0.19mm ± 0.7mm and 0.27mm ± 0.7mm respectively. For the delayed loaded implants, the mean mesial and distal bone levels were 0.14mm ± 0.7mm and 0.09mm ± 0.6mm respectively. No statistically significant differences were found in crestal bone levels over time in the immediately loaded implants compared with the delayed loaded implants (mesial changes in bone levels p=0.70, distal changes in bone levels p=0.12).
CONCLUSIONS: Using bone level changes over time as a criterion to measure implant health, there was no statistically significant difference between immediate and delayed loaded plateau design implants. An increase in bone levels was recorded for both groups. Download PDF - 10/30/07
-
Changes in Crestal Bone Levels Associated with a Bacterially Sealed Screwless 1.5˚ Locking-Taper Implant to Abutment Connection
2007 ACP Annual Session | Scottsdale, Arizona | October, 2007
Sujey Rodriguez-Lozano, DDS
Graduate Prosthodontics, University of Minnesota School of Dentistry
Introduction: The microgap associated with a screw-retained implant-abutment connection is often cited as the reason for crestal bone level changes around dental implant-supported restorations. The design of the implant abutment connection may influence crestal bone loss. The purpose of this study was to evaluate crestal bone levels for 50 bacterially sealed locking-taper implants to abutment connections at 3 periods of time after implant placement.
Methods: A retrospective case series study design was used. The sample (33 patients , 50 implants) was randomly selected from patients who received immediately loaded implants between February 2002 and November 2005. The study measured and compared bone levels on the mesial and distal aspect of the implant-abutment connection at three periods of time: time 1- immediately after implant placement, time 2- at least 7 months (post-integration) after placement and time 3- most recent radiograph available but at least 14 months after placement. Descriptive statistics were use to report the results.
Results: The sample consisted of 33 patients who collectively had 50 immediately loaded implants placed. The mean age of the implants was 2.3 ± .82 years. Mean changes in bone levels on mesial (m) and distal (d) surfaces at time: (1), (2) and (3) were reported as: The mean differences for bone levels on mesial and distal surfaces between time (2) and (1) was: on the mesial, 0.3 ± 0.7 mm and on the distal, 0.4 ± 0.6 mm. The mean differences for bone levels on mesial and distal surface between time (3) and (1) was : on the mesial, 1.0 ± 2.1 mm and on the distal, 1.2 ± 2.1 mm. The mean differences for bone levels on mesial and distal surface between time (3) and (2) was : on the mesial, 0.2 ± 0.7 mm and on the distal, 0.2 ± 0.7 mm.
Conclusion: An increase in mesial and distal crestal bone levels was found during the observation period. This could suggest that the bacterially sealed screwless 1.5˚ locking-taper implant to abutment connection may have an important role in maintaining crestal bone levels around implants of this design. Download PDF - 03/24/07
-
Histomorphometry of Explanted Dental Implants
IADR | New Orleans, LA | March, 2007
J. Lemons, M. Anabtawi, P. Beck, and V. Morgan
Department of Prosthodontics, School of Dentistry University of Alabama at Birmingham
Objective: The significant success (%) and longevities of root form dental implants affords opportunities to evaluate and classify device-to-bone interfaces. These opportunities are based on a small percentage that come to revision. Histomorphometric analyses of human explants permits multiple comparisons including in vitro and laboratory in vivo study outcomes.
Methods: A clinical group (headed by VM) have removed root form implants, where indicated clinically, by Magnitudes of osseous integration from three time periods (about 2, 5 and 10 years) are shown in Figure 2 (A-C) trephine osteotomy. The implant body and bone remain in bloc and specimens were immediately fixed in 10% buffered formalin and transferred with selected records for analysis. Specimens were: macrophotographed, evaluated stereomicroscopically; oriented, embedded; prepared by Exakt® sectioning; stained; and evaluated along longitudinal mid-line thin (20-50 micrometer) sections by Bioquant® imaging for bone quality, quantity, and specific anatomical characteristics.
Results: Eighty* plateau-type design received from one source over the past 3 years. Specimens evaluated by staff and students resulted in: (1) adequate bone for 41 longitudinal section histomorphometric analyses; (2) percent bone integration from 5 to 95% that was not significantly correlated (p>0.05) with in vivo factors other than anatomical location; and (3) interfacial bone structures of a mature and osteonal-type anatomy reported previously1. These results support that dental implant-to-bone interfaces can be stable over time and function with bone remodeling leading to a functional anatomy that is characteristic of the implant design. Comparative analyses with screw-type designs of the same biomaterial are scheduled.
Conclusions: (1) en bloc explants from in vivo functional periods from 3 to 126 months showed osseointegration percentages from 5 to 95%; and (2) the bone anatomy was a mature osteonal type structure, characteristic of plateau type implant designs.
Partial student support from Bicon, Boston, MA is acknowledged.
Lemons, J, J Oral Imp, 2004 and in Davies, J. Ed., Bone Engineering, 2000. Download PDF - 03/24/07
-
Histological Analysis for forty one retrieved dental implants
IADR | New Orleans, LA | March, 2007
Muna Anabtawi, Preston Beck, Al Bartolucci, Vincent Morgan, Jack Lemons
Department of Prosthodontics, School of Dentistry University of Alabama at Birmingham
Objectives: To analyze the anatomy and osseous integration status of the hard tissue interfaces for retrieved implants, and to interpret the clinical status of this specific implant patient population through correlating bone integration status and demographical data.
Methods: Eighty dental implants removed for clinical reasons were retrieved from patients over a 3 year period. Forty one explants were selected for histological analysis because they had adequate bone for longitudinal section analyses. Specimens were processed, embedded in plastic, and thin (20-30 micrometer) ground sections were made along the long axis of the implants. Specimens were stained with Sandersons’ Bone Stain. Blinded histomorphometric analysis was performed to measure the percentage of bone area between the plateaus and the bone/implant contact (BIC). Patient records (gender, date of birth, smoking status, time in vivo, type of implant surface, presence of augmentation, and position of the implants in the jaw) were collected and incorporated into the histomorphometric data; and statistical analysis was performed.
Results: There were no strong associations between any of the clinical, patient and implant variables and the bone area percentage and (BIC). In a multiple regression analysis adjusting for the available data, the anterior position was marginally significantly associated with higher percentage of bone and (BIC) (p=0.067). Performing a simple pair wise correlation, females had higher percentage of bone than males (p=0.0898).
Conclusions: The findings support that the success and failure can be caused by a combination of factors not associated with bone integration status. Revision procedures represent a small percentage of dental implants treatment and this study demonstrates that larger numbers of specimens will be required for statistical significance amongst the variables considered. Download PDF - 03/22/07
-
Investigation of maxillary sinus bone graft healing by MicroCT
IADR | New Orleans, LA | March, 2007
P.M.C. CHOPRA1, M. JOHNSON1, P. BECK1, T. NAGY1, M. MARINCOLA2, and J.E. LEMONS1,
1Department of Dental Biomaterials, School of Dentistry University of Alabama at Birmingham
2Rome, Italy
Objectives: A MicroCT analysis of bone healing quality and quantity subsequent to placement of a reformulated tricalcium phosphate (TCP)* in maxillary sinus ridge augmentation.
Methods: Ten(10) trephined rod shaped human bone cores were obtained from an independent source at three months after the placement of tricalcium phosphate particulate in the maxillary sinus for ridge augmentation prior to implant placement. The samples were immediately stored in 10% neutral buffered formalin. Using SCANCO 40 MicroCT machine, the samples were evaluated at resolutions of 6 and 20µm respectively. The threshold for bone and graft material was determined using visual image, intensity (grey level) and histogram analyses. The density and three dimensional micro architecture of the bone and graft material were analyzed using the software which was interactive with the investigators.
Results: The samples were investigated for micro architecture and density of the bone and graft material. Along with mineral density, the trabecular bone parameters such as Trabecular thickness (Tb Th), Trabecular separation (Tb sp), Structural Model Index (SMI), Trabecular number (Tb no), and connectivity density were obtained for each sample and analyzed ANOVA (p≤0.05). The results obtained at both resolutions (6and 20µm) were comparable, however parameters obtained at 20µm will be used in the future studies including histological, histomorphometrical and scanning electron microscopy comparisons.
Conclusions: MicroCT allowed the study of bone both quantitatively and qualitatively without destroying the samples. These results demonstrated an osteoconductive effect of TCP. The mean bone and graft volume obtained was 25.5 and .43 mm3 respectively; suggesting new bone formation and graft dissolution. These results corroborate independent reports of implants having moved to functional status without failures. The data achieved can be further used to correlate with the values obtained from the traditional histological methods.
*SynthoGraft
Partial student support from Bicon, Boston, MA is acknowledged. Download PDF - 09/30/06
-
Assessment of Periodontal Health Around Integrated Abutment Crowns
AAP Annual Meeting, San Diego, CA, September 2006.
Cheng, K.K., Chuang, S.K., Weed, M., Dibart, S.
Background: The Integrated Abutment Crown™ (IAC) (Bicon, Boston MA) is a cementless, screwless implant-supported crown made from a polyceramic material, which is 80% glass and 20% PEX resin. Unlike the porcelain fused to metal crown (PFM), the IAC restoration is fused to the abutment thus eliminating the presence of a crown/abutment microgap. The purpose of the present investigation was to compare various periodontal parameters in patients with IAC, natural teeth (NT), NT restored with PFMs, and implants restored with PFMs.
Materials & Methods: A retrospective cohort study was conducted on patients evaluated from January, 2003 to April, 2005 at the Implant Dentistry Centre – Faulkner Hospital (IDC-FH), Boston, MA. Natural teeth/implants of these patients were separated into 4 groups: Group 1 (NT), Group 2 (NT/PFMs), Group 3 (implants/PFMs) and Group 4 (implants/IACs). Periodontal parameters including modified plaque index (MPI), sulcus bleeding index (SBI), gingival index (GI), and the average of 6 probing depths (PD) from each tooth or implant (MF, F, DF, ML, L, and DL) were recorded at initial and final examinations. Linear mixed-effects models were used to evaluate the associations between the four groups (the main predictor) and clinical periodontal parameters over the follow-up time. A p-value ≤0.05 was considered statistically significant.
Results: TThe sample included 50 patients (22 males, 28 females) with a mean age of 64.2 years (range = 31.65 - 95.16 years) that were observed over a mean follow-up period of 23.07 months (range of 9.99 -26.28 months). A total number of 375 teeth/implants were divided into: Group 1 (105 NT), Group 2 (63 NT/PFMs), Group 3 (68 implants/PFMs) and Group 4 (139 implants/IACs). The mean changes in clinical periodontal parameters of each group were compared to a reference group (Group 1). Gingival index: Group 3 > 2 > 1 > 4. Average probing depth: Group 1 > 2 > 4 (p<0.05) ≈ 3 (p<0.05). (Difference between group 3 and 4 was not statistically significant.) Sulcus bleeding index: Group 4 > 2 > 1 > 3. Modified plaque index: Group 4 (p<0.05) > 2 > 1 > 3.
Conclusion: Group 4 had the most significant decrease in GI compared to the other groups and performed similarly to Group 3 in terms of probing depths. There were no statistical differences with respect to mean change of SBI among the four groups. Group 4 was found to have a significantly higher MPI score compared to Group 1. Further studies evaluating the plaque composition will be necessary in the near future to explain these findings. - 09/23/06
-
An Innovative Immediate Stabilization Technique For Dental Implants
FDI World Dental Congress | Shenzhen, China | September, 2006
Drauseo Speratti, DDS; Meghan Weed, RDH; S.K. Chuang, DMD
Introduction: Several techniques for the immediate stabilization and functioning of dental implants have been used and described over the years. This study demonstrates how effective this procedure can be done, showing the ease with which quality aesthetic results can be achieved without any additional comprehensive laboratory procedures for the provisional phase. A screwless implant/abutment connection improves the efficiency and effectiveness of the procedures. Regular restorative procedures provide the final restoration.
Materials & Methods: The sample was compose of 505 patients who had a total of 1086 implants placed. We used a retrospective cohort study design including patients who had one or more implants placed using the technique of Immediate Stabilization or Loading between November 1999 and January 2006.
Results: The overall lifetime proportional rate was 91.61%.
Conclusion: This study demonstrates how this technique can be efficient and cost effective, allowing patients to function without the need for removable appliances during healing period, significantly reducing operative time. - 06/30/06
-
Conditional Cox Frailty Predictions Within Clusters for Dental Implant Survival
International Association of Dental Research, Brisbane, Australia June 2006.
Chuang, S.K., Cai, T.
Objectives: The purpose of this study was to conduct conditional and joint predictions for the survival of future dental implants using subject level, implant specific covariate information, and the survival information of other implant(s) for the same subject.
Material and Methods: A retrospective cohort study design was conducted. The cohort consisted of subjects having at least one Bicon implant placed. Covariates information used included smoking status, timing of placement, and implant staging were previously identified using an innovative Cox frailty regression model that adjusted for within subject correlations and heterogeneity of implant failure risks.
Results: The cohort composed of 677 patients with 2349 implants placed. To improve the prediction accuracy, we utilized information on the survival status of existing implants along with the covariates. For illustration, we considered the joint and conditional predictions for the survival of three implants from a single subject who was a non-smoker with immediate implant placement after extraction and one stage protocol. For example, conditional on the first and second implants both surviving for 12- and 60- months given the above parameters, the estimated probability for the third implant surviving for 12- and 60- months was 88.8% (95%CI: 82.4%, 93.0%) and 81.4% (95%CI: 69.5%, 87.7%) respectively. On the other hand, conditional on the first implant surviving for 12- and 60- months, the probabilities that both the second and third implant survived 12- and 60- months were 77.7% (95%CI: 66.3%, 86.0%) and 63.1% (95%CI: 45.0%, 75.2%) respectively.
Conclusion: Conditional and joint survival predictions within subjects are challenging and commonly encountered in dental research. The application of this innovative flexible joint Cox frailty approach allows unique survival predictions about implant failure based on prior information about the survival status of other implants within the same subject. - 06/29/06
-
Survival Analysis of Immediate Stabilization Loading of Screwless Dental Implants
IADR General Session | Brisbane, Australia | June 2006
D. Speratti1, M. Hirayama1, M. Weed1, and S.-K. Chuang2, 1Implant Dentistry Centre, Boston, MA, USA, 2Harvard School of Public Health, Massachusetts General Hospital, Chestnut Hill, MA, USA
Objectives: The study's objective was to evaluate the survival rate and to identify covariates (risk factors) for failure of an innovative and efficient technique for immediate stabilization and loading of dental implants with a locking taper connection.
Methods: To address the research objective, we used a retrospective cohort study design including all patients who had one or more implants placed using the technique of immediate stabilization / loading at Implant Dentistry Centre at the Faulkner Hospital, Boston, MA between June 1999 and October 2005. Covariates for failure were grouped into the following categories: demographics, implant-specific, anatomic, prosthetic, and reconstructive categories. The outcome variable was implant failure defined as explantation. Overall implant survival was evaluated by the Kaplan-Meier analysis and risk factors by the Cox proportional hazards models adjusted for clustered failure time observations.
Results: The sample was composed of 506 patients who had a total of 1099 implants placed. The overall Kaplan-Meier survival rate at 12 and 24 months were 90.0% and 88.6% respectively. The overall lifetime success rate without follow-up time adjustment was 91.6%. Covariates associated with implant failure (p < 0.15) in the univariate analysis included: implant position, diameter, well size, length, and coating of implant. Based on the adjusted multivariate Cox model including age at implant placement and gender, covariates associated with implant failure were implant position, length, and presence of coating on the implant (p < 0.05).
Conclusions: There are many advantages with the use of immediate stabilization and loading implants. The overall one-year survival of the immediate stabilization and loading implant system was 90.0%. After controlling for other variables, implant position (posterior jaw) was associated with an increased risk for implant failure while increased implant length and presence of surface coating on the implant were associated with a decreased risk for implant failure. - 10/07/05
-
Immediate Stabilization of Implants for General Dentists
ADA Annual Meeting | Philadelphia, PA | October, 2005
Speratti, D.
Immediate stabilization and function of dental implants has become a preferred method of treatment. Clinical research and engineering improvements have allowed clinicians to offer the treatment more frequently. Leading practitioners utilize the method of “Immediate Loading or Stabilization”. This presentation intends to show a predictable and affordable technique for general practitioners so that they may be able to achieve aesthetic results without additional surgical procedures. Clinical pictures will be presented. - 08/25/05
-
Immediate Stabilization & Function of Dental Implants
FDI Annual Meeting | Montreal, Canada | August, 2005
Speratti. D., Hirayama, M.
Abstract: Immediate Stabilization and Function (ISF) of dental implants has become a preferred method of treatment. Clinical research, engineering improvements, and patients’ needs have allowed clinicians to offer the treatment more frequently. Leading practitioners utilize the method of “Immediate Loading or Stabilization”; however, many clinicians are still skeptical about its success.
Materials and Methods: In this on-going clinical study of 405 fin-type implants (Hydroxylapatite and Titanium Plasma Spray), 142 patients were treated from November 1998 to July 2004 by means of the ISF. All implants were immediately stabilized by fabrication of a temporary prosthesis bonded to natural dentition or splinting implants to one another.
Results: During this period of time, 128 implants successfully integrated and were restored. 14 failed to integrate and were replaced.
Conclusion: With this technique, a clinician may provide immediate temporary restorations of implants in function at the same time of implant placement without additional risks impacting the success of treatment. - 03/11/05
-
Fit of Fixture/ Abutment Interface of Internal Connection Implant Systems
AO Annual Meeting | Orlando, FL | March, 2005
Kim, C., Gwangju, Chung.
Objective: The purpose of this study was to evaluate the machining accuracy and consistency of implant/ abutment/screw combination of internal connection type.
Materials and Methods: In this study, each two randomly selected internal implant fixtures from ITI, 3i, Avana, Bicon, Friadent, Astra, and Paragon system were used. Each abutment was connected to the implant with 32 Ncm torque value using a digital torque controller or tapping. All samples were cross-sectioned with grinder-polisher unit (Omnilap 2000 SBT Inc) after embedded in liquid unsaturated polyester (Epovia, Cray Valley Inc.) Then optical microscopic and scanning electron microscopic (SEM) evaluations of the implant-abutment interfaces were conducted to assess quality of fit between mating components.
Results: 1. Generally, the geometry of the internal connection system provided for a precision fit of the implant/abutment interface. 2. The most precision fit of the implant/abutment interface was provided in the case of the Bicon System which has no screw. 3. The fit of the implant/abutment inte3rface was usually good in the case of ITI, 3i and Avana system and tha amount of fit of the implant/ abutment was similar to each other. 4. The fit of the implant/ abutment interface was usually good in the case of Friadent, Astra and Paragon system. The case of Astra system with the inclined contacting surface had the most intimate contact among them. 5. Amount of intimate contact in the abutment screw thread to the mating fixture was larger in assembly with two-piece type which is separated screw from abutment such as Friadent, Atra and Paragon system than in that with one-piece type which is not separated screw from abutment such as ITI, 3I and Avana system. 6. Amount of contact in the screw and the screw seat of abutment was larger in assembly of Friadent system than in assembly of Astra system than in assembly of Astra system or Paragon system.
Conclusion: Conclusively, although a little variation in machining accuracy and consistency was noted in the samples, important features of all internal connection systems were the deep, internal implant-abutment connections which provide intimate contact with the implant walls to resist micromovement, resulting in a strong stable interface. From the results of this study, further research of the stress distribution according to the design of internal connection system will be required. - 03/11/05
-
Morphological and Chemical Assessment of Two Thin-film Ion Beam Assisted Deposited Bioceramic Coated Surfaces on Ti-6Al-4V Implants
AO Annual Meeting | Orlando, FL | March, 2005
Coelho, P.G., Lemons, J.E.
Nanotechnology has strongly affected biomaterials science and engineering, once reduced condensed matter domains may deeply alter biomaterials electronics properties and thus their in-vivo behavior. It has been shown that nano-thick Ion Beam Assisted Depoisted (IBAD) bioceramic coatings increase osteoblatic activity at early implantation times, and studies have indicated higher bone-biomaterial interfacial shear strength values for IBAD coated implants. The purpose of this study was to morphologically and chemically assess 2 types of IBAD bioceramic coatings and correlate these evaluations to their in-vivo performance. Control (C) and nano-thick IBAD (IBAD 1, IBAD 2) implants were morphologically evaluated on a SEM under various magnifications, following by survey and site-specific EDS elemental assessment. Superficial layer chemical analyzes were performed by XPS (survey and site-specific), and Ca/P ratios were calculated from spectra output. Results showed no evidence of bioceramic coating presence on all implants (IBAD 1, IBAD 2 –too thin for SEM detection), although ion beam assisted surface etch was evident for IBAD implants. EDS showed the presence of Ti and Al for all specimens, and Ca and P presence for IBAD 2 implants only. XPS spectra showed the presence of Ti, Al, C, O and Si for C implant surfaces, Ti, Al, C, O, Si, Ca, and P for IBAD 1 implant surfaces, and C, O, Si, Ca, and P for IBAD 2 implant surfaces, revealing absorbed molecules (Si and C) for all implants and higher thickness for IBAD 2 implants. Stoichiometry ratios were 1.5 and 2.2 for IBAD 1 and IBAD2 respectively. According to the results obtained, IBAD 2 coatings were thicker than IBAD 1, and both were in the nanorange thickness. Stoichiometry ratios revealed that IBAD 1 and IBAD 2 were different than crystalline HA, suggesting that IBAD coating dissolution rates are potentially higher than crystalline HA. These findings were consistent with animal experiments, where biological response increases were detected at early implantation times due to coating dissolution. Coating nanothickness also allowed direct bone contact to implant metallic substrate, as per histological analyzes, as thin coatings disappear as a function of time in-vivo. IBAD coatings physico/chemical characteristics were desirable features for implant biomechanical fixation competence. - 03/10/05
-
Gingival Tissue Health Around Locking-Taper Implant-Abutment Connections
IADR General Session | Baltimore, MD | March, 2005
Coelho, P.G., Materials Science & Engineering, Birmingham, AL, USA, Geurs, N.C., University of Alabama, Birmingham, USA, Freire, J.N.O., Universidade Federal De Santa Catarina, Florianopolis, Brazil, Coelho, A.L., UNICENP, Curitiba, Brazil, and Speratti, D., Faulkner Hospital, Boston, MA, USA
Objective: to clinically/histologically evaluate gingival tissue around locking taper connected implants in a beagle dog model.
Materials and Methods: Six beagle dogs were acquired 12 weeks prior to surgical procedures. Five weeks prior to euthanization, left mandibular 4th premolars were extracted, followed by immediate placement of two 3.5 mm diameter by 8 mm length endosseous implants at the mesial and distal root sockets. Locking taper abutments were installed to distal implants and the flap was closed by standard suture techniques. Three weeks prior to euthanization, locking taper abutments were installed on left mandibles mesial implants and the same surgical procedure previously described was used to place an implant of same dimensions on the mesial root socket, followed by abutment installation. All surgical procedures were followed by a single dose AB protocol. No mechanical/chemical plaque control was performed, and a crunchy diet was utilized throughout the study. After euthanization, mandibles were retrieved and abutments removed from implants. 5 µm thick soft tissue sections were obtained in the bucco-lingual direction aiming implants' long axis central region (H. and E. stained).
Results: Periodic clinical evaluations revealed absence of inflammation signs. Histological sections resembled healthy mucosal tissue for all 18 specimens. The junctional epithelium was well organized and void of intra cellular spaces. Neutrophils were found and few lymphocytes were noted. No vascular proliferation apical to junctional epithelium was observed.
Conclusion: Histological sections revealed that gingival tissue around locking taper connected implants were consistent with healthy gingival tissue. - 03/10/05
-
Biomechanical Performance of IBAD Thin-Coated Implants at Early Implantation Times
IADR General Session | Baltimore, MD | March, 2005
Coelho, A.L., UNICENP, Curitiba, Brazil, Coelho, P.G., University of Alabama at Birmingham, Birmingham, USA, Freire, J.N.O., Universidade Federal De Santa Catarina, Florianópolis, Brazil, Suzuki, M., University of Alabama at Birmingham, Birmingham, USA., IADR General Session; Baltimore, MD
Desirable features of bioceramic thin-coated implants include controlled composition and thickness plus enhanced adhesion to metallic substrates. Also, metallic substrate exposure with subsequent bone direct contact to the implant surface as a function of time in-vivo may be a potential advantage compared to commercially available bioceramic coatings. Objective: compare the mechanical fixation of Ion Beam Assisted Deposited (IBAD) coated implants versus a non-coated grit-blasted/acid-etched (Control) treated implant surface. Methods: three male adult beagle dogs received 2-4 cylindrical implants on the proximal tibiae following sterile procedures. Left and right limbs provided specimens that remained for 5 and 3 weeks in-vivo respectively. After euthanization, the limbs were retrieved by sharp dissection, the implants received a connecting screw in order to adapt to a torque testing apparatus installed in a universal testing machine. Implants were torqued at a 0.5 in/min rate and maximum loads to interfacial failure were recorded. ANOVA was performed with Max Torque as the dependent variable, and time in-vivo and surface type as independent variables at 95% level of significance. Results: no post-surgical inflammation/infection was observed. Radiographic evaluation revealed bone contact to implant for all groups. Surface treatment had a significant effect on maximum torque value, IBAD= 79.55±7.21 N·cm and Control= 62.76±6.37 N·cm. Time in-vivo did not have a significant influence on maximum torque value, 3 weeks=62.52±6.66N·cm and 5 weeks= 67.23±6.9 N·cm. Conclusion: According to the results, IBAD coated implants presented higher anchorage values compared to control implants, supporting favorable conditions for early functional loading of these implants. - 10/01/04
-
Evaluating the Bacterial Seal of an Implant-Abutment Connection
AAP Annual Meeting | Orlando, FL | October, 2004
Dibart, S.
Background: In the submerged implant design, the quality of the implant-abutment connection is thought to play a critical role in preserving the alveolar crestal bone levels from loss due to oral bacteria. Oral microorganism that would colonize that structure are suspected to initiate inflammation and promote bone loss over time. Methods: In order to test the efficacy of an implant-abutment seal to the bacterial challenge in vitro, a 2 phase experiment was devised. Phase 1: testing the ability of the seal to shield the implant well from outside bacteria. 10 abutments were seated on 10 wide body implants and then immersed in culture tubes containing a bacterial mixture. They were incubated for 24 hours anaerobically at 37°C. The abutments were then separated from implants, carbon coated, and the inside well analyzed for bacteria presence using a scanning electron microscope. Phase 2: testing the ability of the seal to prevent bacterial seepage out from the implant well. 0.1µl of a bacterial mix was deposited at the apical end of abutment posts, which were then carefully inserted into implant wells. The implant/abutment units were immersed, individually, in culture tubes containing a sterile broth and incubated anaerobically at 37°C for 72 hours. The broths were then plated on agar plates to check for bacterial growth.
Results: Phase 1: Scanning electron microscopy did not show any evidence of bacterial presence into the implant wells. Phase 2: There was no evidence of bacterial growth on the agar plates.
Discussion: The tested implant abutment seal was hermetic to oral bacteria in vitro, with no microorganisms transiting from the "outside-in" or the "inside-out". - 10/01/04
-
Aesthetic Dental Implant Restorations
ADA General Session | Orlando, FL | October, 2004
Speratti, D.
Aesthetic restorative procedures on dental implants are known to be complexes and difficult to achieve, challenging clinicians and concerning patients where aesthetic is paramount to their needs. The technique shown in this presentation allowed the clinician to insert a screwless and cementless crown into a dental implant with no gap between the crown and the abutment, bringing an immediate aesthetic result. Clinical pictures will be shown in this presentation. - 09/01/04
-
Comparison of the Periodontal Performance of the Integrated Abutment Crowns, Porcelain Fused to Metal Crowns and Teeth: A 2-year retrospective Cohort Study
Oral Presentation OSSEO | September, 2004
Urdaneta, R., et al.
The Integrated Abutment Crown (IAC) is a technique for the fabrication of single-tooth implant-supported restorations where the abutment and the crown material are one integral unit without the use of any screws or cement. There is no clinically discernible interface between the veneer material and the implant abutment due to a chemical bond. The precision of the prosthetic margin has been shown to be more important for the maintenance of gingival health than its location above or below the gingival margin (Richter and Veno, 1973). It was hypothesized that the gingival tissues would respond positively to a restoration without a crown margin. Purpose: The purpose of this 2-year retrospective clinical study was to compare the periodontal health around Integrated Abutment Crowns, Implant and tooth-supported metal ceramic crowns and adjacent natural teeth. Materials and Methods: 221 implants placed in 62 patients, with a mean age of 58.2 years, 56% were placed in the maxilla and 44% placed in the mandible. Of the prosthetic restorations, 151 were Integrated crowns, 70 were implant-supported Metal ceramic crowns, and 65 were tooth-supported metal ceramic crowns. Patients were recalled and the following periodontal measurements were obtained: Gingival index, modified plaque index, sulcular bleeding index and pocket depth. Results: The 2-year survival rate for Integrated crowns was 98.56%. Two Integrated crowns were removed, one due to implant failure. No significant differences in gingival inflammation and sulcular bleeding were observed between Integrated abutment crowns and unrestored teeth notwithstanding the higher plaque accumulation observed around the Integrated crowns. Furthermore, Metal ceramic crowns on implants had the highest bleeding index and the difference between the Integrated crowns was statistically significant. Teeth, regardless of restoration type, had lower pocket depths than implants. Conclusion: The gingival response around the integrated abutment crowns was similar to the health of the marginal tissues surrounding unrestored teeth. There was significantly less bleeding upon probing around Integrated abutment crowns than around implant supported metal ceramic crowns, this may be explained by the absence of a cement interface on the integrated crowns. - 08/01/04
-
A Photoelastic Stress Analysis of Fixed Partial Dentures with Bicon Implants on Mandibular Posterior Area
Korean Acad Prosthodont. | August, 2004
Kang, JU., Kim, NY., Kim, YL., and Cho, HW.
Statement of Problem: Several prosthetic options are available for the restoration of multiple adjacent implants. A passively fitting prosthesis has been considered a prerequisite for the success and maintenance of osseointegration. Passivity is a particular concern with multiple implants because of documented inaccuracies in the casting and soldering process. One way to avoid this problem is to restore the implants individually, however, the restorations of individual adjacent impants requires careful adjustment of interproximal contacts.
PURPOSE: The purpose of this study was to compare the stress distribution pattern and amount surrounding Bicon implants with individual crowns and splinted restorations.
Material and Methods: A photoelastic model of a human partially edentulous left mandible with 3 Bicon implants(4*1 mm) was fabricated. For non-splinted restorations, individual crowns were fabricated on 3 abutments (4.0*6.5 mm, 0 degree, 2.0 mm post, Bicon Inc., Boston, USA) After the units were cemented, 4 levels of interproximal contact tightness were evaluated: open, ideal (8 micrometershim stock drags without tearing), medium(40 micrometer), and heavy(80 micrometer). Splinted 3-unit fixed partial dentures were fabricated and cemented to the model. Changes in stress distribution under simulated non-loaded and loaded conditions(7.5, 15, 30 lb) were analyzed with a circular polaricope.
Results: 1. Stresses were distributed around the entire body of fin in Bicon implants. 2. Splinted restorations were useful for distribution of stress around implants especially with higher loads. 3. By increasing the contact tightness between the individually restored three implants, the stress increased in the coronal portion of implants.
ConclusionsS: Ideal adjustment of the contact tightness was important to reduce the stresses around individually restored Bicon implants. - 03/20/04
-
Biomechanical Evaluation of a Wide Diameter Bicon Dental Implant in Various Bone Conditions
AO Annual Meeting | San Francisco, CA | March, 2004
Bozkaya, D., Muftu, S. and Muftu, A.
An association between higher implant failure rates and regions of poor bone density, commonly found in the posterior maxilla and mandible, has been reported in the literature. Moreover, implant placement in posterior regions is often limited by anatomic changes due to edentulism, where implant design alteration may be an alternative for treatment planning. In this regard, using a short implant with a large diameter in anatomically compromised regions may provide further increase in implant stability and long-term clinical success. The purpose of this study was to evaluate the biomechanical response of the bone for a wide and short implant, (WSI) (6 mm in diameter x 5.7 mm in length) versus a narrow and long implant (NLI) (3.5 mm x 11 mm) in various bone densities through finite element analyses (FEA). Both implants are using Bicon Morse-taper and made of Ti-6AL-4V. The implants and their respective bone domains were graphically designed through 3-D CAD software. After mesh refinement, different cortical to trabecular ratios and elastic moduli were assigned to the bone domain's elements to reproduce various bone conditions (Types II-IV). Vertical and horizontal loads were applied to the top of the Morse-taper connected abutments of the two implants. Implant and bone stress and strain states were evaluated numerically for analysis. The results showed that the implants presented comparable strain distributions under vertical loads and that the WSI presented lower strain values when the horizontal load was considered. The stress invariant values were also lower for the WSI implant. Increased stress and strain values were found at lower bone densities, where these values were higher for the NLI in most cases. According to the results obtained by this computer-based analysis, it can be concluded that the WSI implant presented an overall better biomechanical force distribution than the NLI when horizontal forces were applied for the different bone densities analyzed and may be considered for implantation of anatomically compromised regions and regions of poor bone quality. - 03/10/04
-
Bacterial Adhesion on Integrated Abutment Crowns™. In Vivo Study (II)
IADR/AADR/CADR 80th General Session | Honolulu, HI | March, 2004
M. MARINCOLA, S. DIBART, M.L. WARBINGTON, Z. SKOBE, R. URDANETA, and S.-K. CHUANG, University of Cartagena, AISI, Italian Association of Restorative Implant Dentistry, Rome, Italy, Boston University, MA, USA, Forsyth Institute, Boston, MA, Harvard University, Concord Dental Associates, Concord, MA, USA, Massachusetts General Hospital and Harvard School of Dental Medicine, Harvard School of Public Health, Chestnut Hill. IADR/AADR/CADR 80th General Session; Honolulu, HI
Objectives: The purpose of this study was to compare the subgingival microbiota present on implant supported Integrated Abutment Crowns (IAC) and natural teeth in vivo.
Material and Methods: A cross-sectional study design was utilized with patients selected from the patient pool at the Implant Dentistry Centre at Faulkner Hospital (Boston, MA). Thirty-one patients (13 males and 18 females) were selected, mean age 57.36 years (range 28.09 to 90.85 years) of which 4 were smokers. Selection requirements were: Patients had IAC crowns placed at least 6 months ago and had not taken antibiotics 3 months prior evaluation. Gingival index (GI), modified bleeding index (MBI), subgingival plaque samples and clinical photographs were taken on at least 1 IAC and the natural contralateral tooth on each patient. The subgingival plaque samples were taken from the mesial side of the IAC or natural teeth and put in an Eppendorf tube containing 0.150 ml Tris-EDTA. The samples were then hybridized with 12 whole chromosomal probes to Tannerella forsythensis, Prevotella intermedia, Campylobacter rectus, Fusobacterium nucleatum, Actinomyes odontolyticus, Streptococcus sanguis, Streptococcus intermedius, Actinobacillus actinomycetemcomitans serotype b, Actinomyces naeslundii, Streptococcus oralis, Porphyromonas gingivalis and Prevotella intermedia , using the checkerboard DNA-DNA hybridization method. The descriptive statistics and generalized linear mixed models (GLMM) accounted for intra-cluster correlation within the same patient were utilized using SAS-PC (version 8.2, 2001) Results: IAC were noted to have less GI and MBI compared with natural teeth but were not statistically significant (p>0.05). There were no statistical differences (p>0.05) in all the various colonies count between IAC and the natural teeth.
Conclusions: The IAC showed striking similarities with the natural tooth in terms of subgingival bacteria plaque count and composition. The IAC also showed lower GI and MBI indices.
Supported by a research grant from Bicon (MM, SD), OMSF Foundation Fellowship in Clinical Investigation (SKC). - 03/10/04
-
Bacterial Adhesion on Integrated Abutment Crowns™. In Vitro Study (I)
IADR/AADR/CADR 80th General Session | Honolulu, HI | March, 2004
S. DIBART, M. MARINCOLA, M.L. WARBINGTON, and Z. SKOBE, Boston University, MA, USA, University of Cartagena, AISI, Italian Association of Restorative Implant Dentistry, Rome, Italy, Forsyth Institute, Boston, MA.
Objectives: The goal of the present investigation was to determine if the DiamondCrown material, used to make Bicon's Integrated Abutment Crown (IAC), is less susceptible to harbor/attract bacterial plaque than All Ceramic (AC) or Metal Ceramic (MC) crowns. A secondary goal was to compare the composition of the plaque attracted on tested surfaces.
Methods: 6 IAC, 6 AC and 6 MC crowns were equally divided in 2 test groups. The AC and MC crowns were cemented on titanium abutments. Group I (3 IAC,3 AC, 3 MC) and group II were incubated for 10 min in a bacterial solution containing 10 different oral bacteria at O.D.1: Tanerella forsythensis, Prevotella intermedia, Campylobacter rectus, Fusobacterium nucleatum, Actinomyces odontololyticus, Streptococcus intermedius, Actinobacillus actinomycetemcomitans serotype b, Actinomyces naeslundii, Streptococcus oralis, Porphyromonas gingivalis. After a brief wash in PBS to eliminate the unbound plaque, the crown samples in group I were incubated in 500µl of Tris-EDTA buffer with 500µl of NaOH. The samples were then hybridized with 10 whole chromosomal probes to the above mentioned microorganisms. The microbiological analysis was completed using the checkerboard DNA-DNA hybridization method. The samples in group II were briefly washed in PBS and fixed in 4% formalin for scanning electron microscopy (SEM).
Results: All experimental crowns showed bacterial adhesion. There was no statistical difference in the microbial compositions when comparing crowns. The SEM showed that the AC crowns were harboring the heaviest bacterial deposits. MC and IAC showed the least bacterial deposits especially at the abutment/crown interface.
Conclusions: The IAC and MC crowns appear to be less prone to bacterial colonization, in an in vitro setting then an all ceramic crown. IAC and MC crowns harbored very few bacteria at the abutment/crown interface.
This study was supported by a research grant from Bicon. - 03/10/04
-
Two-Year Retrospective Evaluation of a Unique Restoration for Single Implants
IADR/AADR/CADR 80th General Session | Honolulu, HI | March, 2004
R. URDANETA, Harvard University, Concord Dental Associates, Concord, MA, USA, M. MARINCOLA, University of Cartagena, AISI, Italian Association of Restorative Implant Dentistry, Rome, Italy, and S.-K. CHUANG, Massachusetts General Hospital and Harvard School of Dental Medicine, Harvard School of Public Health, Chestnut Hill.
The Integrated Abutment Crown™ (IAC) (Bicon, Boston, MA) is a technique for the fabrication of single-tooth implant-supported restorations where the abutment and the crown material are one integral unit without the use of any screws or cement.
Objectives: The objective of this study was to examine the 2-year clinical performance of 151 IACs placed in a general dental practice.
Materials and Methods: A retrospective cohort study design was utilized with patients selected from the patient pool at the Implant Dentistry Centre at Faulkner Hospital (Boston, MA). Patients were recalled and the restorations were evaluated following the modified USPHS criteria. The gingival esthetics and the number of restorative appointments were documented. Descriptive statistics and generalized linear mixed models (GLMM) accounting for intra-cluster correlation within the same patient were utilized using SAS-PC (version 8.2, 2001).
Results: A total of 151 implants were restored with IACs on 59 patients, with a mean age of 58.2 years, 62% were placed in the maxilla and 38% placed in the mandible. The 2-year survival rate for IACs was 98.56%. Two IACs were removed, one due to implant failure; all others were rated as either excellent or good for anatomy, surface texture, and color. No IACs were removed due to fractures. Excellent marginal adaptation was observed with no clinically discernible interface between the veneer material and the abutment. Excellent gingival esthetics was observed. Significantly fewer appointments were needed to restore an IAC than a PFM (p<.0001).
Conclusion: The results of this prosthetic evaluation supported the conclusion that the Integrated Abutment Crown™ is an excellent choice for the restoration of locking-taper single implants for both anterior and posterior areas of the mouth. IACs are a cost-effective and timesaving alternative to PFMs.
Supported by Oral and Maxillofacial Surgery Foundation (OMSF) Fellowship in Clinical Investigation (SKC). - 03/10/04
-
Biomechanical Assessment of an IBAD Surface-Modified Implant
IADR/AADR/CADR 80th General Session | Honolulu, HI | March, 2004
P.G. COELHO, University of Alabama at Birmingham, Birmingam, USA, J. LEMONS, University of Alabama at Birmingham, USA, and A.W. EBERHARDT, University of Alabama at Birmingham, USA.
Attention has been given by implantology research groups regarding thin-film bioceramic coatings on dental implants due to the potential controlled coating dissolution/biological degradation after implantation and direct bone anchorage to the metallic substrate.
Objective: The purpose of this study was to evaluate the biological fixation of a thin-film ion beam assisted deposition (IBAD) surface-modified implant versus a non-surface-modified titanium alloy implant at early implantation times in-vivo in a laboratory canine model.
Methods: The implants were placed in the dogs’ tibiae and remained for 2 and 4 weeks in vivo. After euthanization, the limbs were retrieved and reduced to blocks containing the implant in its center. The blocks were mounted in epoxy resin and the implants were pulled-out at 0.5 in/min in a universal testing machine. Force versus displacement curves were recorded for the specimens, which were subsequently decalcified and prepared (H. and E. stain) for histomorphometric assessment of bone contact at the implant surface enabling interfacial shear stress calculations.
Results: The results showed that bone contact at the implant surface was significantly higher (P<0.03) for the non-surface-modified when compared to surface-modified implants for both times in vivo, and that the pullout forces were not statistically different among the four groups. ANOVA revealed that time in-vivo and surface treatment did not affect interfacial shear stress.
Conclusion: According to the histomorphometric and biomechanical results obtained in this study, it was concluded that there were no weak links between the thin-film coating and the metallic substrate. Furthermore, the bone around the surface-modified implants may have improved mechanical properties, which is a desirable feature for early and long-term implantation of load bearing devices. These results suggest that total dissolution/biological degradation of the coating may not be complete at these early implantation times. - 03/10/04
-
Radial Implant-Abutment Gap Determination Through Serial-Sectioning Method
IADR/AADR/CADR 80th General Session | Honolulu, HI | March, 2004
P.G. COELHO, University of Alabama at Birmingham, Birmingham, USA, M. SUZUKI, University of Alabama at Birmingham, USA, and A.L. COELHO, UNICENP, Curitiba, Brazil.
Significant attention has been devoted by the implantology and bioengineering research community regarding the implant-abutment gap, once such gap may provide a favorable environment for bacterial adhesion/proliferation and to degradation of the metallic substrate. Classically, this distance has been evaluated by means of scanning electron microscopy (SEM) along the implant perimeter and no information is revealed as a function of radius.
Objective: The purpose of this study was to evaluate the implant-abutment gap as a function of radius by means of optical microscopy evaluation through a sequential sectioning technique.
Methods: Six implants (3.75 mm in diameter) and abutments were screw connected and torqued to 20 N.cm. Outer radius measurements were recorded by SEM. The implants were then mounted in epoxy resin using a metallic fixture to assure implant position (perpendicular to the vertical axis). Subsequently, each implant was abraded and polished parallel to its long axis at six different distance intervals. Implant-abutment gaps were obtained by optical microscopy (1000X mag.) and these distances were related to its radial position through trigonometric inferences. A 6th degree polynomial best line fit approach was used to determine the radial adaptation patterns for each of the implants.
Results: The results showed that gap distances were not statistically different among the implants (P=0.05). The polynomial best line fit approach revealed that the implant-abutment gap distance increases as a function of implant radius and this increase is more pronounced in the outer 1⁄4 radius, at the abutment beveled region. Also, communication between external and internal regions of the implant were found for all specimens.
Conclusion: Based on these results, it was concluded that this methodology provided a broader scenario of the implant-abutment gap distance and that SEM evaluations may underestimate the gap value. - 03/01/04
-
Use of Integrated Abutment Crowns to Enhance the Aesthetics of Maxillary Anterior Implant Restorations
AO General Session | San Francisco, CA | March, 2004
Leary, J., Hirayama, M.
Achieving excellent aesthetics with maxillary anterior implant restorations is challenging to even the most accomplished clinicians. Placing implants in the area of the mouth is not only a clinically demanding task but often involves unrealistic patient expectations.
The cases presented here utilize an Integrated Abutment CrownsTM(IAC), an innovative technique in implant prosthetics, to achieve aesthetic restorations in a narrow edentulous space. These cases also demonstrate a multi-disciplined approach solving the problem of esthetics in the maxillary anterior. Orthodontic tooth movement , periodontal plastic surgery, and immediate stabilization have been used to achieve the desired clinical results.
This presentation should add to our ability to enhance anterior aesthetics in even the most demanding situation. - 03/01/04
-
Risk Factors with Radiographic Bone Loss in Dental Implants in a Five-Year Retrospecitve Cohort Study
AO General Session | San Francisco, CA | March, 2004
Chuang, S.K.
Objectives: The purpose of this study was to examine the long-term follow-up (> 5 years) of radiographic evaluation of Bicon dental implants and the risk factors associated with radiographic bone loss beyond the first thread placed at the Implant Dentistry Center (IDC) in Boston, Massachusetts.
Materials and Methods: To address the research purpose, a retrospective cohort study design was used. The cohort was composed of patients who had at least one Bicon dental implant placed for 5 years and were willing to return to IDC for the 5 year follow-up radiographic examination of these originally placed implants. Risk factors were categorized as demographic, implant-specific and anatomic variables. The outcome variable as failure was bone loss beyond the first implant thread on either the mesial or the distal aspects of the implant. Risk factors for bone loss were identified using the generalized estimating equations (GEE) approach adjusted for clustered implant observations within the same patient.
Results: There were 50 patients with 117 implants with a mean age of 50.75 years (range: 17.61 to 82.84 years) of which 26 were females. There were 52 implants placed in the maxilla and 65 implants in the mandible. On the mesial side, 6 implants (5.13%) lost bone beyond the first thread over 5 years. On the distal side, 5 implants (4.27%) lost bone beyond the first thread over the five years. A total of 6 implants (5.13%) had lost bone beyond the first thread on at least the mesial or the distal aspect. Risk factors associated with bone loss beyond the first thread (p < 0.20) included age at implant placement, quality of bone, and implant length. Based on the adjusted multivariate GEE model including gender for biologic importance, risk factors associated with bone loss beyond the first thread was age at implant placement (odds ratio =1.14, p =0.04).
Conclusions: The results of this long-term follow-up radiographic study supported the fact that the Bicon dental implant system is an excellent choice for the prosthetic restoration of the locking-taper implant design. We identified one risk factor (age at implant placement) associated with bone loss beyond the first thread. This key factor is not under the direct control of the practitioner. Supported by Oral and Maxillofacial Surgery (OMSF) Fellowship in Clinical Investigation (SKC). - 03/01/04
-
Immediate Stabilization and Functioning: Anterior Aesthetics
WCOI General Session | Honolulu, HI | March, 2004
Leary, J., Hirayama, M.
The immediate stabilization and loading has become one of the more prominent topics in implant dentistry today. Clinical testing by clinicians, engineering improvements from manufacturers, and patient demand have allowed clinicians to reduce the osseointegration healing period from a conservative time of 6-9 months to period of 1-3 months. Many practitioners acknowledge and utilize the immediate stabilization and functioning: however, a majority of clinicians are still skeptical about such methods and techniques. This presentation shall show step by step methodology of totally chair-side technique of immediate stabilization and functioning with two year retrospective study.
In this retrospective clinical study, 477 fin-type implants (Hydroxyappatite coated, Titanium Plasma Spray, or Uncoated) in 208 patients during the periods from July 1, 2001 unlit July 31, 2003. All implants are immediately stabilized and functioned by fabrication of temporary prosthesis by bonding the prosthesis to remaining teeth or splinting one piece prosthesis for full arch cases.
Further to the normal principles of implant placement the immediate stabilization technique requires only one criterion. That is the ability to prosthetically immobilize the implant with a transitional stabilization prosthesis. Successful osseointegration is not dependent upon the density or quality of the bone to provide initial stability of the implant in its osteotomy. Implants placed immediately after an extraction or even a ridge split osteotomy are excellent candidates for the immediate stabilization or (immediate) loading technique. This technique is applicable for a single implant or for a full arch of implants.
With this new concept and fully chair-side technique shown in this presentation, a clinician can provide an immediately stabilized and immediately functioned prosthesis on the same day as implant placement giving the patient both function and aesthetics. Based upon these clinical evidence, the immediately stabilized and functioned implant technique is a viable treatment option that should be part of every implant practice. - 03/01/04
-
Immediate Loading Implants for Overdentures
AO General Session | San Francisco, CA | March, 2004
Speratti, D.
The immediate loading of implants has become a prominent topic in implant dentistry lately. Engineering improvements from manufacturers and clinical testing have allowed clinicians to offer immediately loaded implants to a wider patient population. The application of this technique for over dentures is a rewarding treatment for both dentists and patients. Patients benefit from gaining immediate prosthetic stability in a cost effective manner and clinicians by being able to offer an efficient and predictable treatment that improves many patients quality of life. - 03/01/04
-
Efficiency Considerations for the Purely Tapered Interference Fit (TIF) Abutments Used in Dental Implants
Journal of Biomechanical Engineering, Trans ASME
Bozkaya, D., Müftü, S. and Müftü, A.
A tapered interference fit provides a mechanically reliable retention mechanism for the implant-abutment interface in a dental implant. Understanding the mechanical properties of the tapered interface with or without a screw at the bottom has been the subject of a considerable amount of studies involving experiments and finite element (FE) analysis. In this paper, approximate closed-form formulas are developed to analyze the mechanics of a tapered interference fit. In particular the insertion force, the efficiency, defined as the ratio of the pull-out force to insertion force, and the critical insertion depth, which causes the onset of plastic deformation, are analyzed. It is shown that the insertion force is a function of the taper angle, the contact length, the inner and outer radii of the implant, the static and the kinetic coefficients of friction, and the elastic modul of the implant/abutment materials. The efficiency of the tapered interference fit, which is defined as the ratio of the pull-out force to insertion force, is found to be greater than one, for taper angles that are less than 6o when the friction coefficient is 0.3. A safe range of insertion forces has been shown to exist. The lower end of this range depends on the maximum pull-out force that may occur due to occlusion in the multiple tooth restorations and the efficiency of the system; and the upper end of this range depends on the plastic deformation of the abutment and the implant due to interference fit. It has been shown that using a small taper angle and a long contact length widens the safe range of insertion forces. - 11/01/03
-
Immediate Loaded implants: How clinicians can achieve aesthetic results
AAID General Session | Hollywood, FL | November, 2003
Hirayama, M., Wang, M.
The “immediate loading” technique has become a popular procedure in implant dentistry. Some practitioners use this method routinely while many remain skeptical about this treatment. The purpose of this study is to demonstrate that the immediate loading technique is a viable and practical treatment option.
Our clinical methodology of “immediate loading” and its concept will be explained in this presentation. Preservation of hard and soft tissue around the implant site is the most critical issue in aesthetic implant dentistry. Clinicians can utilize these methods for many types of cases while providing an immediate temporary restoration on same day implant placement. - 11/01/03
-
Bone Levels around Immediately Loaded-Stabilized Vs. Conventionally loaded locking-taper implants
AAID General Session | Hollywood, FL | November, 2003
Hirayama, M., Urdaneta, R.
Synopsis: Once an implant is uncovered, vertical bone loss of 1.5-2.0mm is observed apically from the newly established implant-abutment interface. This has been well documented for screw-type implant abutment connections.
The purpose of this study was to evaluate bone loss around a locking taper implant-abutment connection interface in immediately loaded and conventionally loaded one and two stage implants. The following objectives will be discussed in this presentation as a retrospective analysis: factors affecting peri-implant tissue conditions; assessment of peri-implant bone levels around immediately loaded vs. conventionally loaded implants; remodeling of peri-implant bone after functional loading; and changes in crestal bone levels during the first year after functional loading.
Download PDF - 11/01/03
-
Mechanics of the tapered interference fit in dental implants
Journal of Biomechanics, Vol. 36, No. 11, pp. 1649-1658
D. Bozkaya and S. Müftü
In evaluation of the long-term success of a dental implant, the reliability and the stability of the implant-abutment interface plays a great role. Tapered interference fits provide a reliable connection method between the abutment and the implant. In this work, the mechanics of the tapered interference fits were analyzed using a closed-form formula and the finite element (FE) method. An analytical solution, which is used to predict the contact pressure in a straight interference, was modified to predict the contact pressure in the tapered implant-abutment interface. Elastic-plastic FE analysis was used to simulate the implant and abutment material behavior. The validity and the applicability of the analytical solution were investigated by comparisons with the FE model for a range of problem parameters. It was shown that the analytical solution could be used to determine the pull-out force and loosening-torque with 5-10% error. Detailed analysis of the stress distribution due to tapered interference fit, in a commercially available, abutment-implant system was carried out. This analysis shows that plastic deformation in the implant limits the increase in the pull-out force that would have been otherwise predicted by higher interference values. - 06/12/03
-
Determination of Bone Activity around a Surface-modified Titanium Alloy Implant
AADR/CADR Annual Meeting | San Antonio, TX | June, 2003
P.G. COELHO, University of Alabama at Birmingham, USA, and J. LEMONS, University of Alabama at Birmingham, USA.
Objective: The purpose of this study was to evaluate the cortical and trabecular bone activity by means of tetracycline bone labeling of a surface-modified (IBAD) versus a non-surface-modified titanium alloy implant in a canine model.
Methods: Implants were surgically placed in the dogs tibiae and the model provided specimens that remained 2 and 4 weeks in vivo. Prior to euthanization, 10mg/Kg oxytetracycline was administered for bone labeling. The limbs were retrieved by sharp dissection, and non-decalcified thin sections containing the implant in their centers were prepared for microscopy evaluation under UV light. Bone activity determination (amount of tetracycline labels) was evaluated dividing the specimens in regions of interest along the length and away from the implant surface (to 2 mm) by quantitative microscopy techniques. Physiologic activity was obtained by tetracycline labeling assessment away (> 3 mm) from the implant surface and comprised the normalizing data.
Results: Results showed that the 4-week surface-modified implant had significantly higher (P = 0.05) amount of tetracycline labeling than other groups and demonstrated that there is significantly more labeling in regions of trabecular bone than in regions of cortical bone. Quantification of the amount labeled for the different regions of interest at different distances from the implant surface (to 2 mm) revealed that the only region that had significantly higher activity than physiologic levels was the region adjacent from the implant surface (to 0.5 mm) and the amount of labeling was significantly higher for the 4-week surface-modified group. Determination of bone activity gradients from the implant surface was performed by linear regression and presented negative slopes from the implant surface.
Conclusions: These results indicated that there is a time-dependent increased osteoconductivity for the surface-treated implants and that increased bone activity after implantation is restricted to the first 0.5 mm region adjacent from the implant surface. - 03/12/03
-
6.0 x 5.7mm Implants: Survival Estimates and Risk Factors for Failure
AADR/CADR Annual Meeting | San Antonio, TX | June, 2003
M.A. GENTILE, S.-K. CHUANG, and T.B. DODSON, Harvard School of Dental Medicine, Boston, MA, USA, Massachusetts General Hospital and Harvard School of Dental Medicine, Boston, USA.
Introduction: Short dental implants facilitate prosthetic restoration in the setting of limited alveolar bone height. Few data exists to support the clinical use of short implants. We hypothesize that 6x5.7 implants are a clinically acceptable option when indicated.
Objective: The study objectives are to: 1) estimate the one-year survival of Bicon 6x5.7 mm implants, 2) identify risk factors associated with 6x5.7 implant failure, and 3) compare the one-year survival of 6x5.7 implants with non-6x5.7 implants.
Methods: We used a retrospective cohort study design and a sample composed of patients having one 6x5.7 implant placed. Predictor variables were categorized as demographic, health status, anatomic, implant-specific, prosthetic, perioperative, and reconstructive. The outcome variable was implant failure defined as explantation. Kaplan-Meier estimates were used to assess implant survival. Appropriate bivariate and multivariate (Cox proportional hazards) survival statistics were computed.
Results: The sample was composed of 35 patients having 172 implants placed (45 6x5.7 and 127 non-6x5.7). The one-year survival of 6x5.7 and non-6x5.7 implants was 92.18% and 95.24%, respectively (p=0.78). Bivariate analyses identified staging and reconstruction as risk factors for failure. After adjusting for covariates in a multivariate model, a single-stage implant placement was found to be a statistically significant (p=0.047) risk factor for implant failure.
Conclusion: We believe this to be the first study reporting on clinical outcomes of the Bicon® 6x5.7 implant. The survival of 6x5.7 implants was comparable to that of non-6x5.7 implants. This data supports the hypothesis that 6x5.7 implants are a clinically acceptable option to facilitate prosthetic restoration in the setting of limited alveolar height. In addition, the results suggest that a two-stage approach is preferred when placing these implants.
Supported by the OMS Foundation Fellowship in Clinical Investigation (S-KC), NIH-NIDCR K24 DE00448 (TBD), MGH Department of OMS Research Fund (MAG). - 03/12/03
-
Mixed-effects Frailty Failure Time Methods to Estimate Dental Implant Survival
AADR/CADR Annual Meeting | San Antonio, TX | June, 2003
M.A. GENTILE, S.-K. CHUANG, and T.B. DODSON, Harvard School of Dental Medicine, Boston, MA, USA, Massachusetts General Hospital and Harvard School of Dental Medicine, Boston, USA.
Purpose: The purpose of this study was to identify covariate effects associated with implant failure by applying clustered semi-parametric Cox proportional hazards frailty survival methods. To our knowledge, this method has not been described or applied widely in the dental research literature.
Methods: To address the research purpose, we used a retrospective cohort study design. The cohort was composed of patients having one or more Bicon implant(s) placed. Covariates were categorized as demographic, health status, implant-specific, anatomic, prosthetic, perioperative, operative, and reconstructive variables. The outcome variable was implant failure (explantation). Covariates for implant failure were identified using the frailty survival methods adjusted for clustered failure-time observations.
Results: The sample was composed of 677 patients having 2349 implants placed. Covariates associated with implant failure (p < 0.15) included operating surgeon, tobacco use, peri-operative antibiotic use, implant position, implant length, well size, coating of implant, proximity of the implant to adjacent teeth or other implants, immediate implant placement, abutment diameter, prosthetic type, usage of reconstruction procedures, and implant staging. Based on the adjusted multivariate frailty model, covariates associated with implant failure were tobacco use, implant length and staging, proximity of the implant to adjacent teeth or other implants, and well size.
Conclusion: Datasets composed of clustered observations are commonly encountered in dental research. Survival analyses of such datasets are exceedingly challenging propositions. We presented an innovative Cox proportional hazards frailty survival methods with clinical applications to implants as an example. We identified five factors associated with implant failure. Three of these variables, smoking status, well size, and staging of implant placement are under the direct control of the practitioner.
Supported by Oral and Maxillofacial Surgery Research Foundation Fellowship in Clinical Investigation (S-KC), NIH grant K24 DE000448 (TBD) and MGH Department of OMS Research Fund (S-KC, TBD). - 03/01/03
-
Immediate Loading and Stabilization: The Clinical Realities
AO General Session | Boston, MA | March, 2003
Hirayama, M., and Wang, M.
The immediate loading and stabilization has become one of the more prominent topics in implant dentistry today. Clinical testing by clinicians, engineering improvements from manufacturers, and patient demand have allowed clinicians to reduce the osseointegration healing period from a conservative time of 6-9 months to a period of 1-3 months. Many practitioners acknowledge and utilize the latest method of “immediate loading” or “immediate stabilization”; however, a majority of clinicians are still skeptical about such methods and techniques.
In this on going clinical observation and study, 168 fin-type implants (Hydroxyappatite Coated or Titanium Plasma Spray Coated) were placed in 98 patients during the period from November 1998 until September 2002. All implants were immediately loaded by fabrication of a temporary prosthesis by bonding the prosthesis to remaining teeth or splinting a one-piece prosthesis for a full arch case. During this period of time, two implants failed to osseointegrate and were subsequently replaced with new implants.
With this new concept and fully chair side technique shown in this presentation, a clinician can provide an immediately stabilized and immediately loaded prosthesis on the same day as implant placement giving the patient both function and aesthetics. Clinical realities with this on-going study will be shown as well as its methodology. Based upon the results of this on-going study, the immediately stabilized and loaded implant technique is a viable treatment option that should be part of every implant practice.
1. Aires I, Berger J. (2002). “Immediate placement in extraction sites followed by immediate loading; a pilot study and case presentation.” Implant Dent.; 11(1):87-94.
2. Cooper LF, Rahman A, Moriarty J, Chaffee N, Sacco D. (20) “Immediate mandibular rehabilitation with endosseous implants : simultaneous extraction, implant placement, and loading.” Int J Oral Maxillofac Implants. July-Aug;17(4):517-25 - 03/01/03
-
Dental implant complications: Types, frequency, and associated risk factors
IADR/AADR/CADR 80th General Session | San Diego, CA | March, 2003
N. MCDERMOTT, S.-K. CHUANG, V. VEHEMENTE, S. DAHER, A. MUFTU, and T.B. DODSON, Harvard School of Dental Medicine, USA, Boston University Goldman School of Dental Medicine, USA, Tufts University School of Dental Medicine, USA, Massachusetts General Hospital, USA.
Objectives: The purpose of this study was to identify the type, frequency and factors associated with complications following placement of dental implants.
Materials and Methods: To address the research purpose, we used a retrospective cohort study design and a sample derived from patients having Bicon (Bicon, Boston, MA) implants placed at the Implant Dentistry Centre, Faulkner Hospital, Boston, MA between 1992 and 2000. The predictor variables were grouped into demographic, medical history, implant-specific, anatomic, prosthetic, and reconstructive categories. The complication variables were grouped into inflammatory, prosthetic or operative. For each patient, one implant was randomly selected for study inclusion. The Cox proportional hazards regression model was used to identify risk factors associated with implant complications.
Results: The sample was composed of 677 patients with a mean age of 53.5 +/- 13.9 years. The overall frequency of implant complications was 13.9% (10.2% inflammatory, 2.7% prosthetic, 1.0% operative). Most implants (62%) with complications did not fail during the study interval. Variables associated with complications (p < 0.15) were: 1) smoking, 2) prosthetic type 3) implant staging, and 4) use of reconstructive procedures. These four variables, gender and age (6 variables total) were included in the multivariate model. Multivariate Cox proportional hazards regression revealed smoking, implant staging, and use of reconstructive procedures to be statistically associated with implant complications (p < 0.05).Prosthetic type was borderline non-significant (p=0.08).
Conclusion: Factors associated with an increased risk for complications include smoking, implant staging, and use of reconstructive procedures. - 03/01/03
-
Risk factors for dental implant failure: A strategy for the analysis of clustered failure time observations
IADR/AADR/CADR 80th General Session | San Diego, CA | March, 2003
S.-K. CHUANG, Harvard School of Dental Medicine, USA, L.-J. WEI, Harvard School of Public Health, USA, and T.B. DODSON, Massachusetts General Hospital, USA.
Objectives: This study's objective was to identify risk factors associated with failure of dental implants by applying innovative, advanced semi-parametric survival methods that adjust for clustered failure-time observations.
Methods: To address the research objective, we used a retrospective cohort study design including all patients who had one or more implants placed at Implant Dentistry at the Faulkner Hospital, Boston, MA between 1992 and 2000. Risk factors for failure were grouped into the following categories: demographic, health status, implant-specific, anatomic, prosthetic, and reconstructive categories. The outcome variable was implant failure defined as explantation. Overall implant survival was adjusted for clustered failure-time observations. Risk factors for implant failure using a dependence model and applying a marginal approach of the Cox proportional hazard regression model.
Results: The sample was composed of 677 patients who had a total of 2349 implants placed. The overall Kaplan-Meier survival rates at one- and five-years were 95.46% and 90.91%, respectively. Univariate risk factors associated with failure (at p < 0.15) were smoking status, implant position, implant length, well size, coating of implant, proximity of the implant, immediate implant placement, abutment diameter, prosthetic type, and implant staging. Based on a multivariate model that adjusts for correlated observations, five factors were statistically associated with implant failures (p < 0.05): 1) smoking status, 2) implant length, 3) immediate implants, 4) implant staging, and 5) well size.
Conclusions: Managing the issue of clustered or correlated observations within the same subject is a common and challenging proposition in dental research. When selecting risk factors for inclusion in the Cox proportional hazard regression models, we recommend adjusting for dependence among dental implant observations within the same patient.
Supported by NIH grants: K16 DE000275 (SKC), R01 CA56844 (LJW), and K24 DE000448 (TBD). - 03/01/03
-
Stress Distribution Characteristics of Various Implant Systems due to Non-central Occlusal Loads
AO Annual Meeting | Boston MA| March, 2003
Bozkaya, D., Müftü, S. and Müftü, A.
Long-term stability of the dental implants strongly depends on the stress distribution characteristics of the implant-bone interface. The occlusal and masticatory loads acting on the prosthesis are transferred to the implant by means of abutment and result in non uniform stress distribution in the bone. In order to maintain a healthy bone, stresses should be in the range of 1.4-5 MPa. Stresses outside this range have been reported to cause resorption of the bone tissue1. In this study, the stress distribution characteristics of five different implants from Bicon, Ankylos, Astra, ITI and Nobel Biocare subjected to an occlusal load located off the central axis are investigated. The dimensions of the implants were comparable in size; however the thread profiles were considerably different from each other. The 2-D axisymmetric finite element models were loaded by 100 N vertical, 20 N lateral forces and 100 N.mm moment, separately and then the results are superposed to combine the effect of these loads to obtain the stress distribution due to a 102 N occlusal load 1 mm offset to the symmetry axis. The Young’s modulus of the bone was varied between 1 GPa (soft trabecular bone) and 16 GPa (hard cortical bone) in order to be able to investigate the success of the implants in different bone densities. The Bicon and Ankylos implant systems seem to distribute the stresses more evenly when compared to Astra, ITI and Nobel Biocare implants in all bone densities. High localized stresses were found at the tip of the Astra, ITI and Nobel Biocare implants that can lead to crestal bone loss, however stresses generated at the other sites of implant-bone interface were low enough to prevent bone resorption. 1. Rieger M. R, Mayberry M, Brose M. O. Finite element analysis of six endosseous implants. J Prosthet Dent. 1990;63:671-6 - 03/01/03
-
Implant-Supported Overdenture Surgery in the Severely Resorbed Edentulous Mandible: A Clinical Report
AO Annual Meeting | Boston MA| March, 2003
Wang, M.Y. & Hirayama, M.
Implant-supported overdentures are an effective means for restoring the resorbed mandible or maxilla. However, restoring the severely resorbed edentulous mandible with implants presents challenges for both the clinician and laboratory technician. A step-by-step surgical procedure for restoring the resorbed mandible with one implant system will be presented. A comparison of this procedure will be made to the treatment of the same patient using other implant systems.
1. Banton, B. and M.D. Henry (1997). “Overdenture stabilization with ball-and socket attachments: principles and technique.” J Dent Technol 14(7): 14-20
2. Visser, A., M.E. Geertman, et al. (2002). “Five years of aftercare of implant-retained mandibular overdentures and conventional dentures.” J Oral Rehabil 29(2): 113-20
3. von Wowern, N. and K. Gotfredsen (2001). “Implant-supported overdentures, a prevention of bone loss in edentulous mandibles? A 5-year follow-up study.” Clin Oral Implants Res 12(1): 19-25 - 03/01/03
-
Tapered Connection Mechanisms in Dental Implants
AO Annual Meeting | Boston MA| March, 2003
Bozkaya, D., Müftü, S.
One of the critical factors determining the success of a dental implant is the stability and the reliability of the implant-abutment connection. In-screw type implant-abutment connection mechanism is widely used in various implant systems; but high incidences of mechanical complications such as screw loosening, or creep deformation in the screw-implant interface are reported1. Tapered interference fits provide an alternative, reliable connection method2. The pull-out force and the loosening torque are the main design considerations to secure a reliable implant-abutment connection. In this work, the mechanics of the tapered interference fits was analyzed using finite element analysis (FEA). A closed-form analytical solution was also sought to determine the contact pressure distribution in the contact region. The validity of the analytical solution was investigated by comparisons with the FEA for different design parameters. The pull-out force and the loosening torque of the implant-abutment system were determined for different insertion depths. The quality and the quantity of the bone surrounding the implant did not have an effect more than 10%. The elastic-plastic FEA showed that the plastic deformation of the implant limits the increase in the pull-out force. This implies that larger insertion depth does not always mean more pull-out force, or a more secure connection. The pull-out force and the loosening torque of the implant-abutment system was large enough to prevent the long-term abutment loosening. 1. Schwarz. Mechanical Complications of Dental Implants. Clin. Oral Impl. Res. 2000;11:156-158. 2. Müftü A, Chapman R. J. Replacing posterior teeth with freestanding implants: Four-year prosthodontic results of a prospective study. Journal of the American Dental Association 1998;129(8):1097-1102. - 10/01/02
-
Immediate Restorations in Clinical Realities
AAID General Session | Los Angles, CA | October, 2002
Hirayama, M.
Immediate loading has become one of the latest trends in Implant Dentistry, due to engineering improvements, modified clinical techniques, and clinical necessities. Osseointegration time allowances have drained from 6-9 months to 4-6 months, and yet again to 1-3 months, while restoration/loading time allowances of the implant have decreased to immediate 2 weeks. This study presents successful clinical immediate restoration cases on a two component fin-type dental implant, including methodology. - 10/01/02
-
The New Generation In Aesthetic Dentistry: Extra-Oral Cementation & Integrated Abutment Crown™
AAID General Session | Los Angles, CA | October, 2002
Hirayama, M., Marincola, M., Wang, M.
With the flexibility of the Bicon Dental Implant System, the common problems associated with traditional screw and cement retained restorations can be eliminated. By using extraoral cementation you avoid the problems of excess sub-gingival cement. A strong and flexible Integrated Abutment Crown™ can be created without the use of screws or cement. This new restorative concept will provide a superior aesthetic result, while reducing occlusal stress on the dental implant. - 03/01/02
-
Integrated Abutment Crown with Poly-Ceramic Material
Hinman General Session | Atlanta, GA | March, 2002
Wang, M.Y.
Traditionally, there are screw-retained or cement-retained restorations for implant prostheses. These techniques are well known to clinicians. Screw-retained attachments can lead to screw loosening caused by occlusal forces and cement-retained restorations can lead to problems because of excess cement around the subgingival margin. Both of these problems can lead to a significant loss of time and expense for the dentist. A product has recently been introduced which enables a dentist to build the crown directly onto an implant abutment in the laboratory, and subsequently tap the abutment and crown as a unit into the implant well. This technique eliminates the problems of screw-loosening and excess cement subgingivally. This table clinic shows the step-by-step technique of the Integrated Abutment Crown. - 03/01/01
-
Bone Morphology Associated with Biologic Width Among Various Dental Implant Designs
AO General Session | Toronto, Canada | March, 2001
Hirayama, M., and Wang, M.
The design of a dental implant can affect the clinical results of implant treatment. While all designs can achieve a certain level of success, there are specific engineering designs that do not experience the same problems and issues as others. Three problems commonly cited with dental implants are: (1) bone integration levels (2) biological width surrounding implants and (3) the complexity of restorative components. This study compares different implant systems in their bony architectures through various surgical stages. Different implant designs affect the bony morphology differently. These differences can lead to differences in integration strength and the biological width. We found that, in general, one-stage implants and one fin-type implant preserve bone better than the two-stage screw-type implants. A comparison of several dental implant designs and their clinical results is presented here. - 03/19/97
-
Comparison of Ss Penetration Through Various Implant-Abutment Connection Mechanisms
IADR General Session and Exhibition | Orlando, FL | March, 1997
Muftu, A., Chapman, R.J., and Mulcahy, H.L., Tufts University School of Dental Medicine & Suffolk University Department of Biology, Boston, MA.
Bacterial penetration through implant fixture-abutment interface (FA) may vary with the type of the connection mechanism. There appears to be significantly less bacterial penetration with the lock-and-taper mechanism than with most screw type mechanisms. However, design of screw systems differ with implant systems. The objective of this study was to determine whether a difference in microbial penetration exists in: 1) two different FA designs: (i) - lock-and-taper mechanism and (ii) - screw type mechanism and 2) within various screw mechanisms. After determining internal volume of all fixtures, FA-assemblies were attached according to manufacturer’s specifications and autoclaved. The, FA assemblies were immersed in a liquid medium exhibiting heavy growth of Streptococcus sanguis (ATCC 10566) and incubated at 35˚C. After 7 days , samples were rinsed with 25 ml of ultrafiltered, sterile H2O twice. Prior to disassembly, external surfaces were dried with sterile gauze to prevent contamination by the remaining medium along the FA interface. Under aseptic conditions, abutments were removed and, using a 26 G 3/8 in. needle attached to P100 Pipetman micropipering device, the inner parts of fixtures were filled with sterile saline respectively. This suspension was aspirated with the same instrument and inoculated into trypticase soy broth.Implant # Tested # Showed Ss Growth Implant # Tested # Showed Ss Growth Bicon 10 0 IMZ (4.0mm Ø) 7 2 Branemark 11 4 Minimatic 8 2 IMZ (3.3mm Ø) 9 3i 7 0
Statistical differences using Student’s t-test between the implant systems were: Bicon vs. Branemark p<.01; Bicon vs. IMZ (3.3 mm Ø) p<.000; Branemark vs. IMZ (3.3 mm Ø) p<.03; IMZ (3.3 mm Ø) p<.008); Minimatic vs. IMZ (3.3 mm Ø) p<.003; 3I vs. Branemark p<.03; 3I vs. IMZ (3.3 mm Ø) p<.000. Locking taper abutment connectors and one thread design abutment connector appear to resist bacterial penetration in vitro. -
- 03/01/96
-
Comparison of Microbial Penetration Between Components of Screw and Locking Taper Implant-Abutment Connections
IADR General Session and Exhibition | San Francisco, CA | March, 1997
Muftu, A., Chapman, R.J., & Mulcahy, H.L., Tufts University School of Dental Medicine & Suffolk University Department of Biology, Boston, MA.
It has been suggested that the seal between implant fixtures and abutments is not hermetic. There is a potential reservoir for bacterial flux which might play a role in peri-implantitis and/or the outcome of guided tissue regeneration after peri-implantitis. The objective of this study was to determine whether a difference in microbial penetration exists in two different implant fixture-abutment (FA) designs: 1) lock-and-taper mechanism and 2) screw type mechanism. Ten Bicon and 7 Branemark FA assemblies were attached according to manufacturer's specifications and autoclaved. Then, FA assemblies were immersed into a liquid medium that was previously inoculated with Streptococcus sanguis (ATCC 10556) and incubated at 35°C. After 70 hours, samples were rinsed with 25 ml of ultrafiltrated, sterile H2O twice. Prior to disassembly, external surfaces were dried with sterile gauze to prevent contamination by the remaining medium along the FA interface. Under aseptic conditions, abutments were removed and, using a 26G 3/8 needle attached to P100 Pipetman micropipeting device, the inner parts of Bicon and Branemark fixtures were filled with 5 microliters and 15 microliters of sterile saline, respectively. This suspension was aspirated with the same instrument and inoculated into trypticase soy broth. After 42 hrs, 1 out of 10 Bicon and 4 out of 7 Branemark implants showed growth while none of the sterility controls were contaminated. In this study, there appears to be significantly less bacterial penetration with the lock and taper mechanism than with the screw-type mechanisms. (Student's t-test p<0.05). The size of the spaces in the locking taper mechanism may prevent or reduce bacterial downgrowth. - 03/01/94
-
Tissue Interfaces for Titanium Alloy Plateau Implants
IADR General Session and Exhibition | Seattle, WA | March, 1994
Mitchell, S., Lemons, J., & Wellons, H., University of Alabama and Stryker Dental Implants, Kalamazoo, MI.
Previous studies have demonstrated that integrated calcium phosphate ceramic (CPC) coated plateau design root-form implants have a unique distribution and orientation of mineralized phases associated with a vasculature that was specific to the plateau design.1 This study focused on three non-coated Ti alloy plateau implants to determine if similar anatomical characteristics existed. The three specimens consisted of transmitted and reflected light microscopy and contact microradiography. The overall orientation of bone and vasculature was similar to the CPC coated implants (i.e., oriented haversian bone with mid-central positioned vascular channels relative to the plateaus), while the distribution of mature bone was greatest along the apical portions of the implants. A thin layer of non-calcified material was observed between the alloy and bone of one specimen. There was no evidence of inflammation present in any of the specimens. These analyses support previous results and showed that the distribution and orientation of bone integrated with CPC coated and non-coated Ti alloy plateau implants are similar. The bone anatomy for the plateau design is uniquely different compared to screw or rod (bullet) designed root-form dental implants. The importance of this difference related to load bearing capabilities and stability are unknown at this time and will be the subject of extended research.
This study was supported by Stryker Instruments.
1 Mitchell, S.C., Lemons, J.E., Wellons, H, Tissue Interfaces for HA Coasted Dental Implants. Abstract, IADR/AADR General Session and Exhibition, Chicago, March 1993.
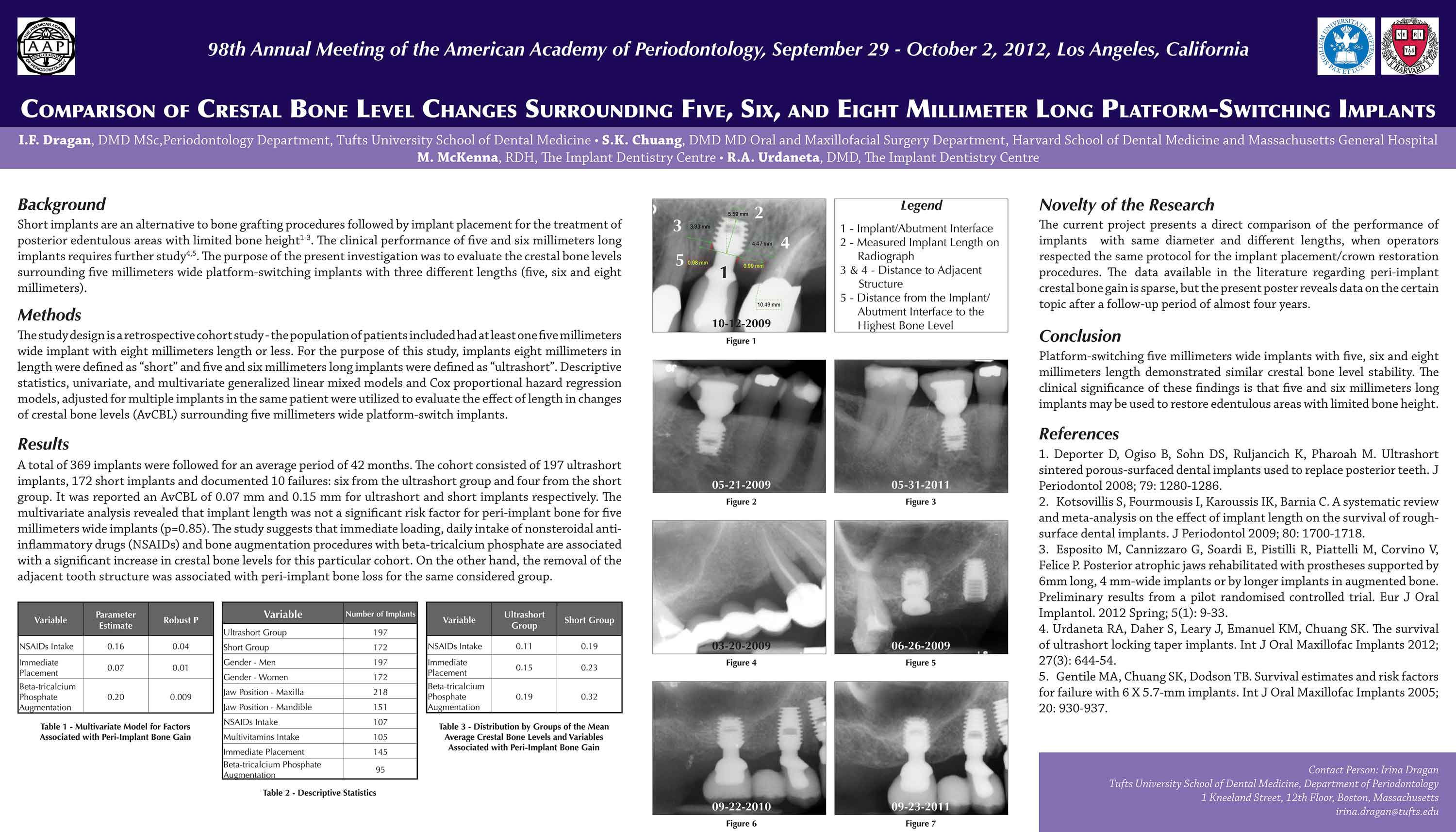{kind=link}